Renal Cell Carcinoma
Understanding the pathological characteristics of
Renal Cell
Carcinoma is essential to plan the imaging strategy
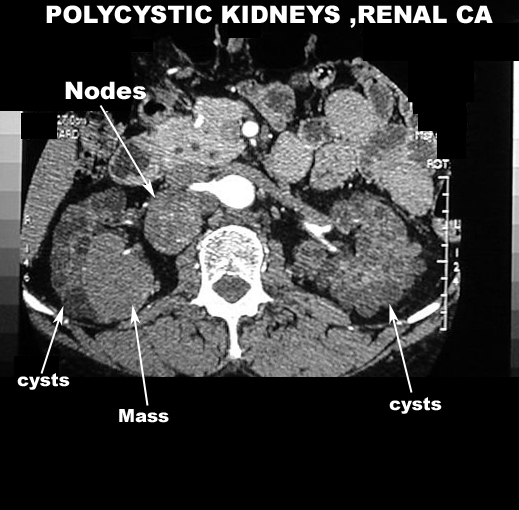
- In can be bilateral in 5% of patients
- Associated with von-Hippel-Lindau disease,
Tuberosclerosis and Polycystic disease
- Presents as mass lesions 3-15 cm in
diameter
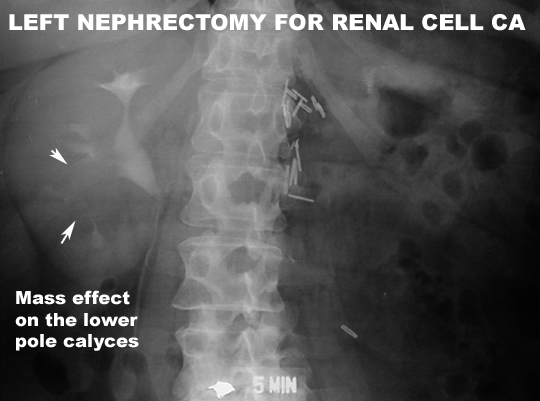
- As they grow they distort renal outline and
grow into renal pelvis and fungate through the walls of the collecting
system into surrounding tissue
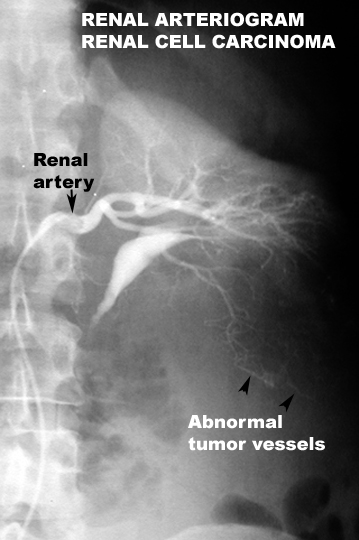
- Tumor is highly vascular
- Tumor becomes necrotic and cystic areas can be
seen.
- There is a tendency to invade renal vein and
extend to inferior vena cava and heart.
- There is a tendency to metastasize widely to
lungs, bones and lymph nodes, liver, adrenals and brain and opposite kidney
Objective for imaging procedures
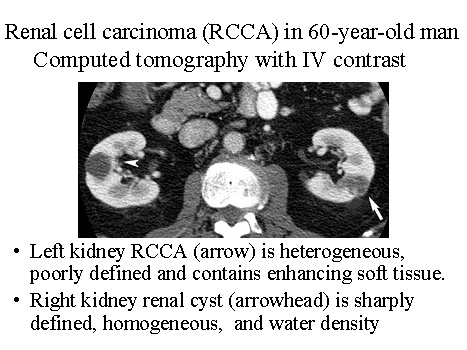
CT abdomen and pelvis with
contrast is the procedure of choice when a renal neoplasm is suspected to
evaluate the mass and stage the tumor.
- Can delineates cysts from solids.
- Can show tumor enhancement.
- May show calcifications
- Can show involvement of renal vein
- Can show involvement of peri-nephric fat
- Can assist with fine needle aspiration biopsy
- Can show metastases to liver, nodes and bones
- Better in showing tumor recurrence
Chest x-ray is a routine initial procedure
looking for metastasis. CT chest is superior in detecting occult metastatic
lesions.
Role of other imaging procedures:
-
MRI:
with contrast is a good alternative when iodinated contrast cannot be used because of renal failure
or when vascular patency and involvement needs to be assessed.
- Ultrasound: is a simple
screening procedure to distinguish a cystic from a solid mass. Vascular
status can also be assessed with Doppler.
- Most masses are hyper echoic; some may be hypo echoic and some may be isoechoic to the parenchyma
- Necrotic mass; may be seen as cystic with thick walls
- IVC involvement with thrombus may be seen
- IVP and renal angiograms
(Neovascularization Image )
are rarely done nowadays. MRI and CT provide all the necessary information about the status of renal vaculature and inferior vena cava.
ADPKD
Renal
cancer MSK
{kind=link}
{kind=link}
{kind=link}
{kind=link}