

|
Infantile spasms represent a variety of generalized, myoclonic seizure characterized by brief motor spasms affecting the trunk and extremities. These movements are similar to the infantile startle reaction and may involve slight flexion or extension movements of varying degrees. Although each individual spell is momentary, spasms may occur up to hundreds of times daily. Spasms are often not immediately recognized as seizures by parents or health professionals due to the unique and fairly subtle motor manifestations.
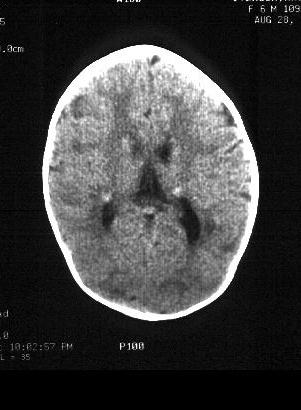
Spasms typically present during the first of life, most often between 4 and 6 months of age. The spasms result from underlying neurologic disease in a majority of cases, with tuberous sclerosis, cerebral dysgenesis, and hypoxic-ischemic encephalopathy the most frequently identified causes.
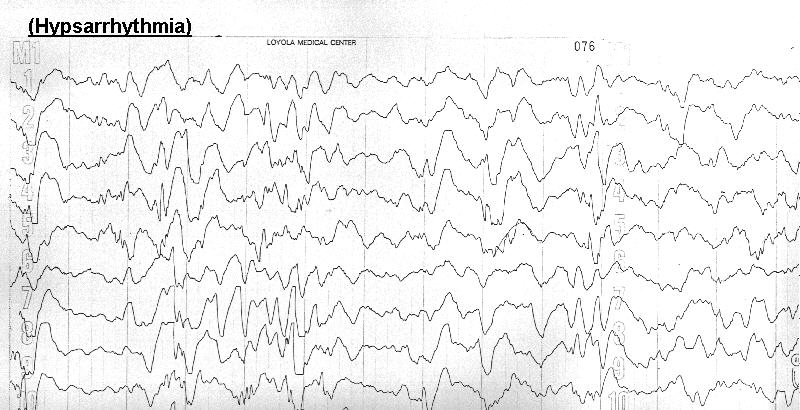
Diagnosis is extablished on the basis of clinical manifestations, although the characteristic EEG finding of hypsarrhythmia is found in up to 80% of cases. Hypsarrhythmia consists of a unique, chaotic pattern of asynchronous, high amplitude slow waves and spikes which is peculiar to this disorder.
Treatment of infantile spasms is problematic, since response to traditional anticonvulsant agents is poor. Parenteral ACTH is generally considered to be first-line therapy. The optimal dose and duration of therapy have not been definitively established, but generally range from 10 to 160 units/m2/day for 4 to 12 weeks (including tapering). Side effects are frequent, including hyppertension, Cushing syndrome, and irritability. High-dose valproic acid or clonazepam may be of benefit in cases refractory to ACTH.
Children with infantile spasms face considerable risks for long term neurologic morbidity. Moderate or severe neurodevelopmental impairment eventually afflicts up to 95% of children with identified underlying causes for their seizures and up to 60% of those with idiopathic spasms.
| thoban@lumc.edu | Last Updated: August 11, 1996 Created: July 25, 1995 |
{kind=link}
{kind=link}