
|
|
Lung Parenchymal Disease |
The lung parenchyma is initially abnormal on chest radiographs in about one-half of patients. The percentage is higher on computed tomography which can detect disease when the radiograph is normal. If lung tissue is obtained, however, there is histologic disease in almost all patients, including those who have no visible lung abnormalities on imaging studies. This is why transbronchial biopsy has such a high diagnostic yield and is the favored means of obtaining tissue for diagnosis.
The involvement of the lung parenchyma by sarcoidosis can have very different appearances ranging from reticulonodular lung tissue densities to multiple masses and miliary lesions. These radiographic expressions of sarcoidosis can mimic many other diseases including malignancies and infections which involve the lungs. There are certain radiologic features, however, that are very useful in limiting the differential diagnosis of lung parenchymal disease in these patients. For example, air containing bronchi in mass like lesions and small nodules distributed along lymphatic vessels are important features of sarcoidosis. These findings are illustrated in this section.
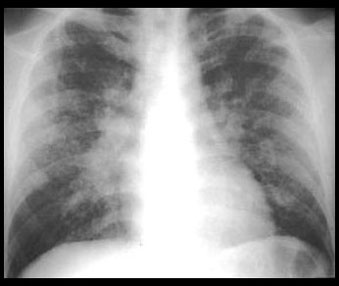
The radiologic patterns of lung disease are produced by interstitial granulomas and associated interstitial densities. Chest radiographs most often show well defined linear and nodular densities which are characteristic of lung tissue disease. Each nodule represents mutiple coalescent granulomas since an individual granuloma is microscopic.
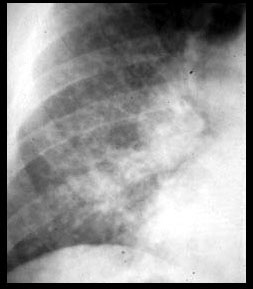
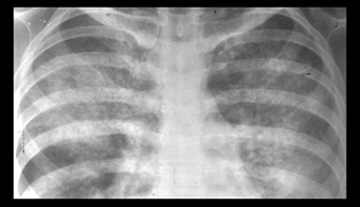
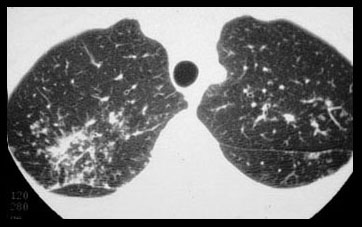
| RETICULONODULAR PATTERN | CLOSEUP OF RETICULONODULAR PATTERN |
|---|---|
|
|
This pattern of widespread interstitial lung disease is a common appearance of sarcoidosis involving the lung parenchyma. Note enlarged hilar lymph nodes. |
Note well defined linear and nodular densities characteristic of lung tissue (interstitial) disease. |
With progession nodules can compress small peripheral airways resulting in poorly defined confluent densities which have an appearance similar to pneumonia and other diseases which fill the alveoli. Larger conglomerations of granulomas can appear as tumor like masses. Miliary and cavitary lesions are rare. Rarely endobronchial nodules or lymphadenopathy obstruct bronchi and cause atelectasis.
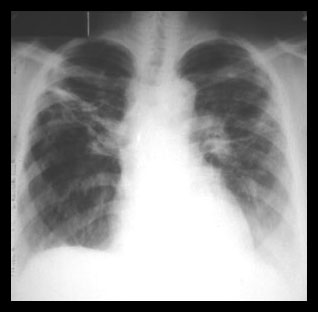
Most parenchymal lung disease resolves. A minority of patients develop irreversible pulmonary fibrosis with disability ranging from minimal to death. This Stage IV disease is often most severe in the upper lobes. The radiographic findings can range from minimal to extensive. These findings include: fibrosis with irregular septal thickening, broad bands and masses of fibrous tissue, traction bronchiectasis, upper lobe volume loss, emphysema, bullae, and honeycomb end stage lung.
Pulmonary fibrosis can lead to cor pulmonale and right heart failure. Bullae can be colonized by fungi, most often anAspergillusspecies. This results in a mobile ball of hyphae in the bulla. The formation of a fungal ball is sometimes preceded by thickening of the wall of the bulla or the adjacent pleura.
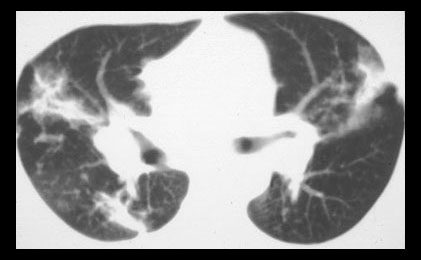
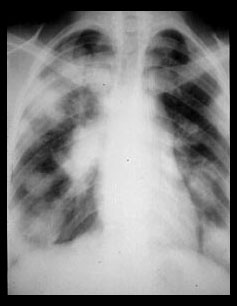
| STAGE IV | STAGE IV |
|---|---|
|
|
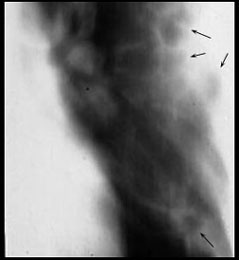
Extensive pulmonary fibrosis is typically worst in the upper lobes as in this patient. |
Computed tomography in Stage 4 sarcoidosis shows broad bands of fibrosis in the upper lobes. |
| ACINAR PATTERN | PNEUMONIC APPEARANCE |
|---|---|

|
|
These poorly defined nodular opacities are the size of pulmonary acini (6mm). |
In this patient confluent acinar opacities look similar to pneumonic consolidation. |
Computed tomography can show disease when radiographs do not and can also better demostrate lymphadenopathy and the characteristic features of sarcoidosis involving the lung parenchyma. This can be important when the diagnosis is uncertain.
The small ( 2-10mm ) nodules are characteristic of sarcoidosis. These nodules are primarily distributed in the lung tissue along lymphatics. Many are located along the bronchovascular bundles, in the subpleural interstitial space beneath the viseral pleura, and in the interlobular septae. These nodules are much easier to see on computed tomography studies than on radiographs. Computed tomography done with thin ( 1-2mm ) sections and the highest spatial resolution possible is known as high resolution CT (HRCT). HRCT is the best way to show details of lung tissue disease, except for small nodules. On 1-2mm sections, blood vessels in cross section are difficult to differentiate from lung nodules.
Several HRCT images following conventional CT imaging are often used to better show lung tissue disease.
Patchy abnormal increased density of the lung with preserved visibility of the underlying anatomy is called ground glass density. Ground glass density is common on HRCT of sarcoidosis but is not specific. It has been hypothesized that in patients with sarcoidosisis this density is due to alveolitis, but there is no convincing proof that sarcoidosis causes alveolitis, and in addition, ground glass density can be produced by lung tissue disease. Ground glass density, however, probably does correlate with active reversible disease.
None of the radiographic or CT findings that can be produced by sarcoidosis are pathognomonic. The small nodules of sarcoidosis are characteristic, but small lung nodules similar to sarcoidosis are also common in lymphangitic lung metastases and silicosis. Lymphangitic metastases to the lung can closely resemble sarcoidosis. Small nodules distributed along lymphatics are common to both. Lymphangitic metastases, however, cause greater septal thickening and less distortion of the lobular anatomy than sarcoidosis. Silicosis is also characterized by small nodules and can look similar to sarcoidosis, but the history and clinical findings are distinctive.
| NODULAR PATTERN | SUBPLEURAL NODULES |
|---|---|

|
|
Small 5mm nodules are usually shown by CT in patients with sarcoidosis. Many nodules are subpleural, along fissures, and as in this patient, along bronchovascular bundles. The nodules give the vessels (arrow) and fissures a beaded appearance. |
The cluster of small nodules here looked like a tumor on a radiograph.
|
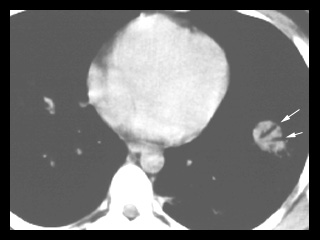
| ALVEOLAR SARCOIDOSIS | ALVEOLAR SARCOIDOSIS |
|---|---|
|
|
Multiple lung masses such as this are an unusual form of sarcoidosis which resembles lung metastases. |
Computed tomography shows a mass which has air containing bronchi (arrows) within it.. In addition to sarcoidosis, bronchioloalveolar carcinoma, lymphoma, and pseudolymphoma can present as a mass with air bronchograms. |
| MILIARY SARCOIDOSIS | CAVITARY SARCOIDOSIS |
|---|---|

|
|
CT shows innumerable well defined lung nodules less than 5mm in diameter. This is a miliary pattern which is rare in sarcoidosis. These lung lesions are indistinguisable from miliary tuberculosis, fungal disease and a variety of other diseases. |
This is the rare pattern of multiple cavitary sarcoid lung lesions. There were cavitary lesions in the right lung also. Note lymphadenopathy . |



| Terrence C. Demos, M.D. |
Last Updated: March 14, 1996 Created: March 1, 1996 |