li-9-1
AUTOIMMUNE HEPATITIS
By Dr. E. Orfei
There
is a group of liver diseases of uncertain etiology, with or without
autoantibodies, with or without hypergammaglobulinemia, which do or do not
respond to steroid therapy. These conditions may be due to an immune disorder.
The list includes:
-Autoimmune
hepatitis.
-Primary
biliary cirrhosis.
-Vanishing
bile ducts.
-Primary
sclerosing cholangitis
-Hepatic
granulomas.
-Graft-versus-host
disease.
Of
the above only autoimmune hepatitis responds to steroid treatment.
Here
we will discuss autoimmune hepatitis The other conditions will be treated in
other sections.
Definition
A
chronic active hepatitis without identifiable etiology in people sometimes
affected by other autoimmune
diseases.autoimmune hepatitis
Clinical
presentation
It
manifests:
-
clinically with malaise and sometimes jaundice.
-
biochemically with elevation of serum transaminases (ALT) and gamma
globulins.
-morphologically
with necroinflammatory changes in periportal hepatocytes (piecemeal necrosis).
-serologically
with presence of autoimmune antibodies and hyprgammaglobulinemia.
The
onset may be acute or gradual, chronic, insidious. It starts with acute symptoms
in 30% of the cases with jaundice, fever, malaise, liver tenderness, like an
acute viral hepatitis. It has insidious onset in the remainder of the cases to
the point that in a large number of cases (30 to 80 %) the disease is discovered
at the cirrhotic stage sometimes already decompensated. It can occur at any age
and in both sexes but it affects mostly women 10 to 30 years old or around late
middle age. F/M ratio is 4:1. Other autoimmune diseases frequently accompany
this type of hepatitis: autoimmune thyroiditis, Sjogren syndrome,
glomerulonephritis, systemic lupus erythematosus, etc.
Serology
Serological
tests are used to investigate the presence of autoimmune antibodies. There are
two classes of autoantibodies: non-organ specific and
organ specific.
The
non-organ specific are:
ANA,
antinuclear.
SMA,
antismooth muscle.
ANTIACTIN.
LKA1,
liver kidney microsomal 1.
These
antibodies are easily assayed and are present in 20 to 80% of patients with
autoimmune hepatitis, but they are not specific for liver antigens.
The
liver-specific antibodies are:
ASGPR,
anti-asialoglycoprotein receptor antibodies.
They have high specificity for immune hepatitis (88%), but they occur also in 7%
of hepatitis B, 8% of alcoholic liver, 14% of primary biliary cirrhosis and
in 82 % of patients with anti-ANA and
anti-SMA. Therefore ASGPR has more diagnostic value than ANA and SMA.
LP,
anti-liver-pancreas antibodies. Present in 33%
of patients may by the sole positive antibodies in an occasional case.
LC1,
anti-liver cytosol type 1. Prevalent in
patients younger than 20 years. Very frequent in children. Typically absent in
children with acute fulminant autoimmune hepatitis. It supports the diagnosis of
autoimmune hepatitis.
SLA,
anti-soluble liver antigen
which
is represented by cytocytic keratin 8 and 18, highly specific for autoimmune
hepatitis
Clinical
Subclassification.
Based
on immunological findings, 3 types of this disease have been proposed.
Type
1: positive for anti- ANA, SMA, Antiactin. It is the
most common type in U.S.A. More typical of women. Hypergammaglobulinemia in 97%
of patients. It may have fulminant onset and may be discovered at the stage of
cirrhosis.
Type
2: positive for anti-LKM1. Predominantly in children.
Rare in adults in U.S.A. Patients have more extrahepatic immunologic diseases,
lower gamma globulins and higher tendency to develop cirrhosis despite steroid
therapy.
Type
3: positive for anti-SLA. Rare in U.S.A. (3%). Most
affected young females (20-40). It may rapidly progress to cirrhosis.
Variations
Thirteen
per cent of patients have the clinical and histological disease but lack
immunoserologic markers.
for
sub classification. These cases are classified as cryptogenic chronic
hepatitis or autoantibody-negative autoimmune hepatitis. They are
indistinguishable from type 1 autoimmune hepatitis and respond well to steroid
therapy.
Pathology
The
vulnerable area affected by autoimmune hepatitis is the periportal region. There
is marked portal and periportal chronic inflammation with lymphocyte and
macrophages which spill through the limiting plates encircling periportal
hepatocytes,("rosetting") which are destroyed,("piecemeal
necrosis")."Bile duct lesion"
may
be present (damaged portal bile duct surrounded by a massive lymphocytic
reaction).
Connective
tissue replaces the lost parenchyma. The portal tract is expanded and assumes
a"maple leaf"configuration. Periportal necrosis and
fibrosis may extend far rom the portal region and link with an adjacent portal
tract forming a bridging necrosis. Cirrhosis may follow. This process is similar
to any other chronic active hepatitis. Only the presence of an excessive number
of plasma cells and the rosetting phenomenon may indicate an autoimmune process,
but their scarcity or absence do not rule out this condition. The histological
form of lobular hepatitis especially in relapses is a distinguishing finding
from viral hepatitis
 |
 |
 |
 |
|
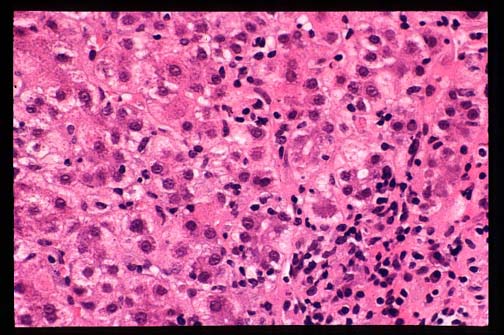
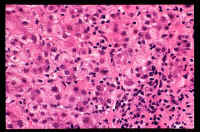
Fig.
9-1-1-Autoimmue
hepatitis.
A
portal field with chronic inflammatory cells, mostly lymphocytes and
plasma cells. In this hepatitis, contrary to viral hepatitis plsma c
present in a significant number.
|
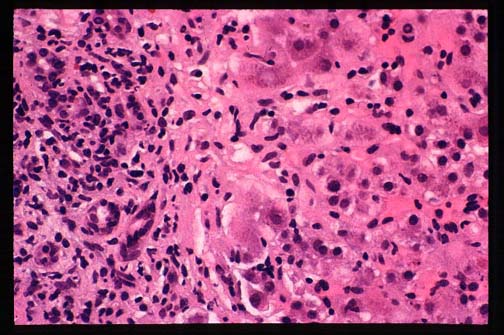
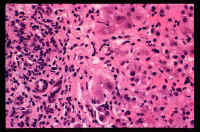
Fig.
9-1-2-Autoimmune hepatitis.
Periportal
piecemeal necrosis with chronic
in
inflammation, plasma cell reaction and
portal
fibrosis.
|
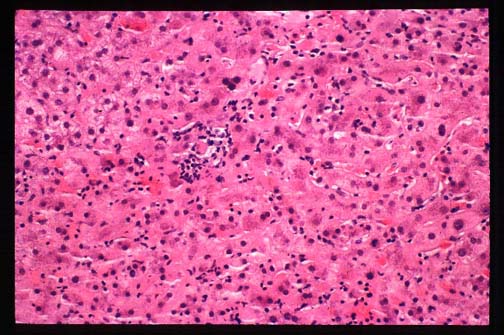
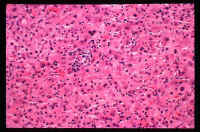
Fig.
9-1-3-Autoimmune hepatitis.
Lobular
inflammation and focal necrosis.
|
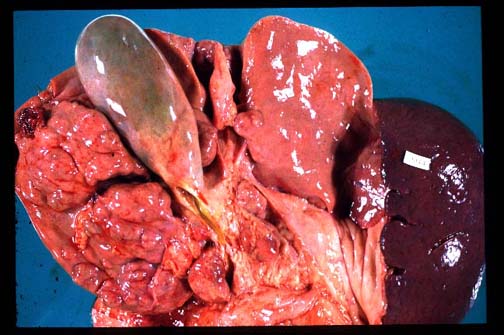
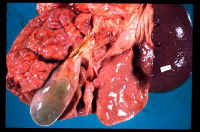
Fig.
9-1-4-Autoimmune hepatitis.
Cirrhotic
stage. This patient was a 16 year old
girl
affected by hepatitis for only 3-4 years.
Notice
the macro nodular appearance of the
liver
very similar to viral hepatitis.
|
Diagnosis
The
following criteria are suggested for diagnosis by the International
Autoimmune Hepatitis
Group:
-normal
serum levels of alpha-1-antitrypsin, copper and ceruloplasmin.
-seronegativity
for IgM anti-viral hepatitides.
-seronegativity
for cytomegalo and Epstein-Barr viruses.
-no
parenteral blood exposure.
-low
ethanol ingestion.
-no
recent use of hepatotoxic drugs.
-any
serum aminotransferase abnormality.
-serum
gamma globulin, IgG, >1.5% normal.
-ANA,
SMA or LKM1 >1:80 in adults and >1:20 in children.
-liver
biopsy to rule out other lesions.
In
any suspected case an early diagnosis is mandatory in order to establish the
earliest treatment.
Treatment
The
treatment consists of steroids with or without azothioprine. Not all cases need
to be treated.
Absolute
treatment is needed when:
-transaminases
are 10 fold normal;
-transaminases
5 fold normal and serum globulins twice normal.
-Bridging
necrosis
-Multilobular
necrosis
-Incapacitating
symptoms
No
treatment is needed:
-
minimum transaminases and/or globulin levels.
-minimum
or no symptoms.
-inactive
cirrhosis.
-liver
failure with mild inflammatory activity.
-severe
treatment complications.
Liver
transplantation. At least 2 weeks of therapy should be
attempted before deciding transplantation. Patients with multilobular necrosis
and unimproved hyperbilirubinemia require expeditious transplantation.
Prognosis
Remission
in 55% of patients after 2 years of therapy. Ten year life expectancy in 90%
with or without cirrhosis.
Relapse
occurs in 50% of patients 6 months after drug withdrawal. Re-treatment induces
remission.
Failure
occurs in 9% of patients.
Maximum
possible response consists of some but no
complete response in 3 years of therapy.
Readings:
Czaja A J, Medical Clinics of North America, 80:973-994, 1966.(100 references)
CONTENTS