
|
|
Other Organ Systems
The liver is usually involved if biopsied, but only about 1/3 of patients have hepatomegaly or biochemical evidence of disease. Symptoms are usually absent, but cholestasis, fibrosis, cirrhosis, portal hypertension, and the Budd-Chiari syndrome are rare outcomes which have been documented.
Acute polyarthritis with fever is a common presentation of sarcoidosis and when there is accompanying erythema nodosum in a patient with bilateral hilar lymphadenopathy this is LOFGREN'S SYNDROME. The arthritis ranges from mild with no physical findings to severe with swelling and tenderness. The arthritis is self limited and usually lasts for weeks to months. Chronic destructive bone disease with deformity occurs but is rare.
Muscle disease is rare. A chronic myopathy affecting the proximal limb muscles can lead to weakness and wasting which is similar to muscular dystrophy. This usually affects postmenopausal women. Two even less frequent forms of sarcoidosis are acute myositis and one or more granulomatous nodules of muscle.
The conducting system and left ventricular myocardium are primarily effected. Heart dysfunction is most often due arrythmias, conduction abnormalities, or cardiomyopathy. If sarcoidosis has not been previously diagnosed, patients may present with findings which indicate some type of obscure heart disease. There may be chest pain, intractable arrythmias, or heart failure without an evident etiology. Sudden death has been reported.
The central nervous system, cranial nerves, and peripheral nerves can be involved. The cranial nerves are most often effected, and peripheral seventh nerve facial palsy is the most common neurologic manifestation of sarcoidosis. This is usually acute, transient, and can be unilateral or bilateral. When unilateral the picture is similar to idiopathic Bell's palsy. When accompanied by fever, uveitis, and enlargement of the parotid gland this presentation of sarcoidosis is called HEREFORDT'S SYNDROME. Other cranial nerves can be involved alone or along with the seventh nerve.
Optic nerve sarcoidosis can produce papilledema. Lesions of the pituitary and hypothalamus have caused diabetes insipidus and deficient pituitary hormones.
Paresthesias and decreased reflexes due to peripheral nerve lesions are frequent but are easy to overlook. Mild deficits are usually asymmetric and scattered. The findings can resemble multiple sclerosis.
Meningeal granulomas are common, but meningeal symptoms are not.
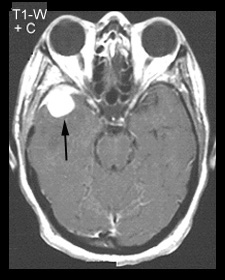
Central nervous system involvement can produce encephalopathy and granulomatous masses produce the signs and symptoms of a neoplasm or other space occupying lesion. This is illustrated by the following patient.
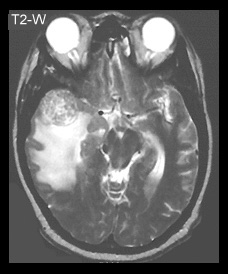
| T1-W POST GADOLINIUM MR IMAGE | T2-W MR IMAGE |
|---|---|
|
|
This post contrast image shows a high signal intensity temporal lobe sarcoid lesion (arrow) |
This image shows high signal intensity edema surrounding the biopsy proven sarcoid lesion. |
Rarely granulomatous interstitial nephritis produces renal failure which develops over a period of weeks to months. Most have a rapid response to steroid therapy. Kidney stones (nephrolithiasis) are very unusual as is deposition of calcium in the kidney parenchyma and collecting tubules (nephrocalcinosis). Both are the result of the hypercalcemia and hypercalciuria associated with sarcoidosis.
Aside from the salivary glands, the alimentary tract is rarely involved. Sarcoidosis of the stomach can narrow the antrum and cause pyloric obstruction. The lesion is similar to other granulomas including Crohn's disease and also mimics adenocarcinoma. Rare small intestinal and colon lesions can resemble Crohn' disease or carcinoma.
The prognosis of sarcoidosis is good in most patients. The majority of patients with acute disease recover completely. Those patients who do have residual damage of affected organs usually have only minimal organ dysfunction. A small minority of patients have persistent active, recurrent, or chronic disease leading to disability or death. Organs at greatest risk are the lungs, eye, heart, and central nervous system.
In the small number of patients who are treated, steroids are the therapy of choice. Other medications have used, but none have been proven to be more effective than steroids. The decision to treat is especially difficult since sarcoidosis resolves spontaneously in most patients and, in addition, late fibrotic changes may not be affected by therapy.


| Terrence C. Demos, M.D. |
Last Updated: March 14, 1996 Created: March 1, 1996 |