What are the useful imaging modalities used to investigate a renal mass?
Ultrasonography
The initial imaging procedure of choice, US can distinguish between a cyst and from a solid mass. Three major criteria for a single simple cyst on ultrasound are:
the mass is round and sharply demarcated with smooth walls
no echoes (anechoic) within mass
strong posterior wall echo indicating good sound transmission through the cyst
No further evaluation is necessary if all of these criteria are satisfied, since the likelihood of malignancy is small.
If US equivocal, or suggestive of malignancy
solid or complex
with internal echoes
and irregular walls
if calcifications or septae are seen
if multiple cysts are clustered so that they may be masking underlying carcinoma
Then proceed to CT
CT
A renal CT scan both with and without IV contrast is the next appropriate step.
It has replaced the renal arteriography as the next diagnostic step.
CT is as accurate as, and obviates the potential morbidity of, angiography in defining the renal mass.
Also, CT can give information about local staging to allow definitive surgical management if needed.
MRI
MRI is used to evaluate solid tumors seen on CT if a patient is unable to receive IV contrast.
Vascular invasion, IVC thrombi are demonstrated without IV contrast.
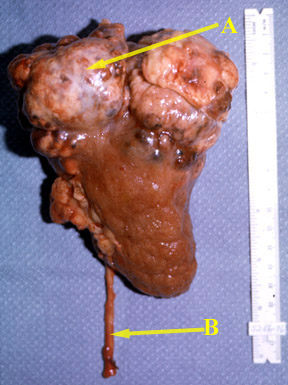
What are the pathological characteristics of renal cancer?
Mass in kidney
Propensity to invade renal vein and inferior vena cava
Tumor can extend to perirenal structures - nodes
What are the useful imaging procedures in patients suspected to have renal cell carcinoma?
We will discuss the primary tumor and not investigation of metastatic lesions.
Primary tumor
CT is the diagnostic procedure of choice. It can provide information about the mass, perirenal extension, vascular invasion, nodal and liver involvement.
US: Serves as a screening test to diagnose renal cysts.
MR: Useful to evaluate vascular invasion by the tumor.
IVP and angiogram are rarely used now.
Metastatic workups
What are the imaging manifestations of renal carcinoma?
CT
Hypodense unless it is hemorrhagic
Cystic mass
Calcified mass
Most enhance after contrast administration, but less than normal kidney enhancement
Thickened or irregular walls of cystic portion
Thickened or enhanced septae within the cystic mass
A multilocular mass
Invasion of renal vein and IVC
Nodes
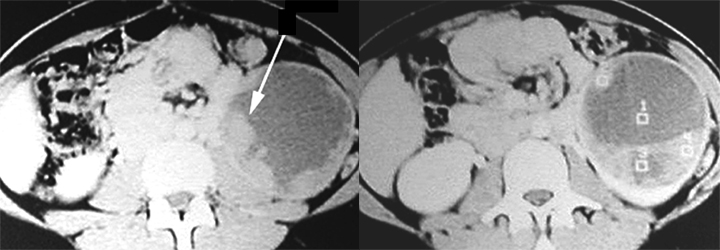
Renal Cell Carcinoma
Arrow: Solid hypodense mass left kidney
Arrowhead: Normal parenchymal enhancement.
Renal Cell Carcinoma
Mass is cystic and solid.
Tumor nodules are seen arising from the wall of the cyst pointed
by long arrow.
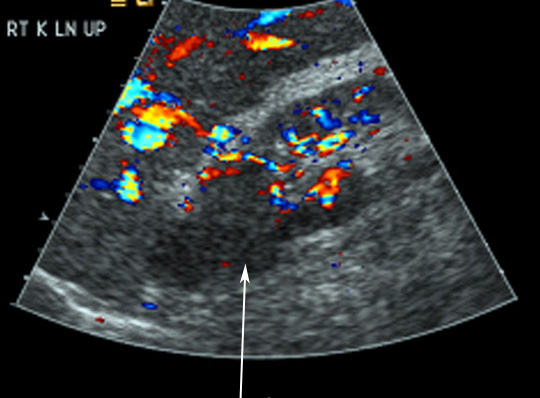
US
Iso echoic mass or hypoechoic mass
Hyperechoic mass
Renal Cell Carcinoma
Almost isoechoic mass from upper pole
No posterior wall enhancement to suggest a cyst.
MR
T1: Low signal
T2: High signal
Enhances with contrast
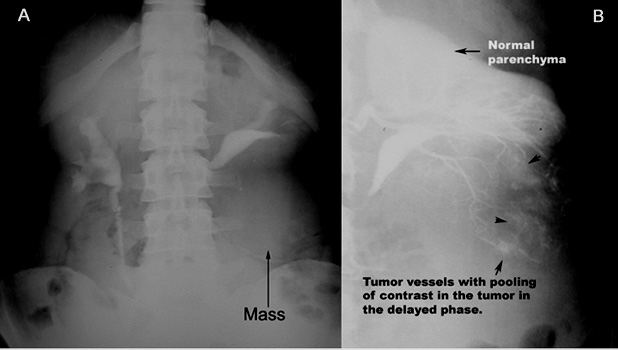
Angiogram
Neovascularization
Renal Cell Carcinoma
A: IVP shows mass in the lower pole of left kidney. B: Angiogram showing neovascularization.
Sensitivity, specificity and complications of fine needle aspiration biopsy (FNAB):
Fine needle aspiration biopsy can be performed with ultrasound guidance.
Fine needle aspiration has limited value in the evaluation of a renal mass.
The sensitivity and specificity of FNAB for a renal cell carcinoma is 80-95%.
Therefore, 5-15% of renal cell carcinomas are missed in FNAB.
FNAB is reserved for the diagnosis of abscess, with concomitant drainage tube placement, or cancers such as lymphomas, which are medically, not surgically, managed.
Complications include bleeding, infection, needle tract seeding, arteriovenous fistula, and pneumothorax.