
The liver is flabby, soft, friable similar to any acute viral hepatitis. It was called in the past
"acute yellow atrophy".
|
Li-84 DRUG-INDUCED LIVER INJURY by Dr. Emilio Orfei |
INTRODUCTION
Hundreds of drugs are hepatotoxic. We know the mechanism of action on the liver only for few drugs. They attack this organ at different sites. The hepatotoxicity is produced through two mechanisms: toxic metabolites and immunological reaction. Indeed some drugs will continue to damage the liver after their suspension.
Many drugs of every pharmacological group are involved. When a drug reaction is suspected, the literature of administered drug must be reviewed.
PATHOLOGY
Each drug produces different morphological and functional alterations an therefore different clinical manifestations. The morphologic lesions are:
-Hepatitis
, acute and chronic, sometimes indistinguishable from viral hepatitis with hepatocellular necrosis, inflammation, cholestasis. It can be acute and sometimes hyperacute and fatal (fulminant) or it can be chronic with fibrosis and even cirrhosis. Observed with: Amineptine,Nitrofurantoin, Phenybutazone, Quinidine,Sulphonamides.and many more.
-Cholestasis
without inflammation or necrosis. The cholestasis is intralobular, cytoplasmic and canalicular mostly of zone 3. It is attributed to impairment of bile secretion from the hepatocyte into the bile canaliculus for an acquired defect of the bile secretory apparatus of the hepatocyte similar to the congenital defect in Dubin-Johnson syndrome. The prognosis is good with suspension of the drug. Sometimes resumption of the drug after some time does not cause any more the cholestatic reaction.Drugs involved:
Oral contraceptives, estrogens, anabolic steroids. Chlorpromazine.-Cholestasis with portal inflammation
. Changes similar to previous cholestatic picture plus non-specific portal inflammation..Observed with:
Captopril, Azothioprine, Chlorpromazine, Gold, Cyclosporine, Erythromycin, Penicillamine..
-Cholangitis( affecting portal bile ducts) and Cholangiolitis(affecting portal bile ductules).The mechanism is probably immunoallergic. There is epithelial degeneration of bile duct epithelium, neutrophlic infiltration in and around bile ducts or ductules, portal lymphocytic and eosinophilic reaction The lesions are usually reversible with discontinuation of the drug but permanent rarefaction of bile ducts may result with some drugs with changes similar to primary biliary cirrhosis: Example:
Chlorpromazine.-Granulomatous
hepatitis. These granulomas are always non-caseating, intralobular or portal or both. They may be clinically silent. They may produce elevation of serum alkaline phosphatase due to small multi focal parenchyma compressions affecting the bile flow.Drugs involved:
Allopurinol, Aspirin, Diazepam, Isoniazide, Phenitoin, Sulphonamides.Steatosis,macrovesicular:
Presence of single, large fat droplets in hepatocytes pushing the nucleus to the periphery of the cell, with or without necrosis (pyknosis). This change is probably due to impaired egress of lipid from hepatocyte. The cell cannot export any more its lipoproteins.Drugs involved:
Glucocortocoids, Methotraxate, L-Asparaginase.Steatosis, microvesicular: presence of small fatty vesicles filling the cytoplasm of the hepatocyte (foamy hepatocyte). The nucleus is in the center of the cell. The lesion is attributed to interference with oxidation of fatty acids by mitochondria. Very serious lesion. Seen in azotemia, pancreatitis and acute steatosis of pregnancy. Some responsible drugs are: Tetracycline, Pirprophen, Amineptin, Valproate.
Phospholipidosis:
there are foamy hepatocytes plus, under electron microscopy, large lysosomal inclusions composed of densely packed concentric membranes with a fingerprinting pattern. There is also reduction of the crystae in the mithochondria and vesicles in the smooth ER. The lesion was recognized by Oda in Japan in 1969. Later, in 1975, it was recognized by Lullman et al in inborn errors of phospholipid metabolism. Drugs responsible: Colargil (Oda et al. 1969), Amiodarone (Pousell et al.1984).-Vascular lesions
: venous thromboses, necrotizing angiitis, arterial intimal hyperplasia,perisinusoidal fibrosis (Vit.A), sinusoidal dilatation, peliosis, veno-occlusive disease,
Budd-Chiari syndrome, hepatoportal sclerosis, nodular hyperplasia of the liver.
Drugs:
Immunosuppressive drugs, oral contraceptives, testosterone.-Hepatic tumors
: hepatocellular adenoma and carcinoma, cholangiocarcinoma, angiosarcoma, hemangioendothelioma.Drugs:
Anabolic and contraceptives drugs, Vinyl Chloride.
EXAMPLES\
|
HALOTHANE HEPATITIS |
Case History
Forty four year old lady hah uterine curettage for metrorrhagia. Eight weeks later she had hysterectomy. Three days after hysterectomy she became jaundiced. Seven days later she died in liver failure. Halothane was used as anesthetic in both surgical procedures. The autopsy showed massive liver necrosis. It appears that the liver damage was mediated by an immunoreactive mechanism. Multiple exposures increase the incidence of liver damage.
|
Fig.8-4-1:Fulminant
halothane Hepatitis.
The liver is flabby, soft, friable similar to any acute viral hepatitis. It was called in the past "acute yellow atrophy".
|
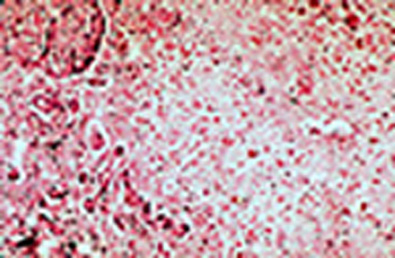 |
Fig.8-4-28-4-2. Histology of the same case.
Massive centrolobular necrosis. Notice the central vein and necrosis of liver cells in all three zones of the lobule. A few cloisters of hepatocytes in form of cords and pseudo-ductules remain in the periphery of the lobule.Notice absence of inflammatory reaction and no endophlebites of the vein as it would be seen in viral hepatitis.
|
|
Fig. 8-4-3. Chlorpromazine (Thorazine)
With this drug 1% of patients are prone to develop jaundice which appears after 1-5 weeks of treatment. The hepatic damage consists ofcytoplasmic and canalicular cholestasis with mild portal inflammation with eosinophils.Cytonecrosis is minimal. Prognosis is good. Notice the presence of fine yellow granular bilepigment in the cytoplasm of hepatocytes around the central vein (zone 3).
|
|
AMIODARONE HEPATITIS |
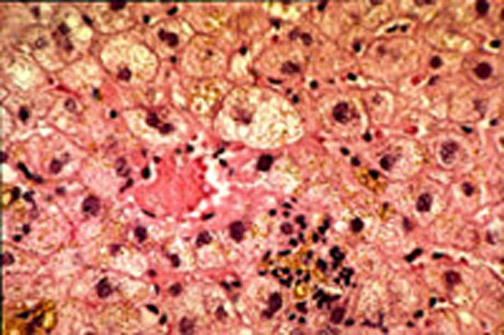 |
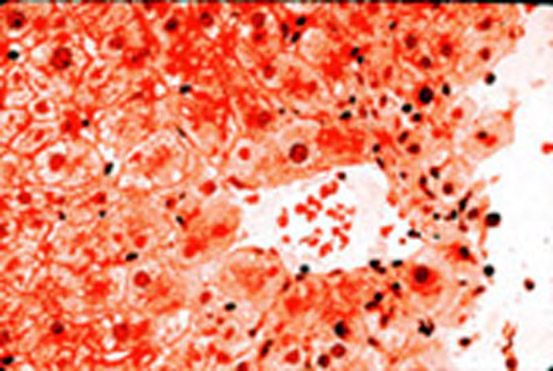
Fig. 8-4-4 Amiodarone hepatitis 54 year old male taking amiodarone for many years developed clinical hepatitis: ALT 780, AST 339. This slide demonstrates hydropic swelling of hepatocytes, focal cell necrosis with inflammatory reaction and cytoplasmic cholestasis. The foamy appearance is due to phospholipidosis
|
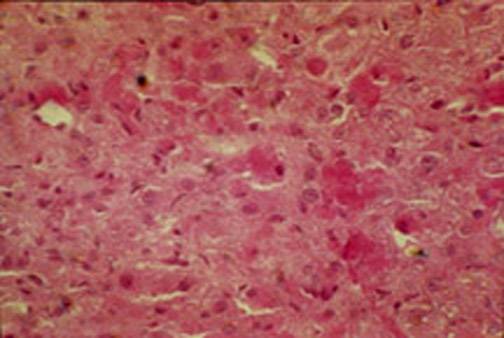 |
Fig.8-4-5. Same case.(AMIODARONE)
This drug produces also Mallory bodies in the periportal area.
|
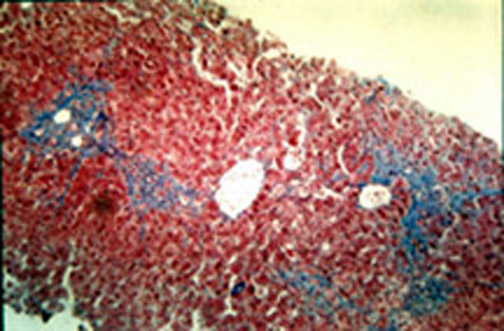 |
Fig.8-4-6. Same case. In this case, which is longstanding, there is beginning portal, periportal and porto-central fibrosis.
|
|
Phenytoin (Dilantin) This anticonvulsivant drug which commonly causes lymphadenopathy, polyarteritis nodosa and bone marrow damage rarely affects the liver. Here it can cause cholestasis multifocal necrosis, lymphocyte "beading"in sinusoids similar to infectious mononucleosis but more commonly it causes multiple histiocytic granulomas which cause high elevation of serum alkaline phosphatase.
|
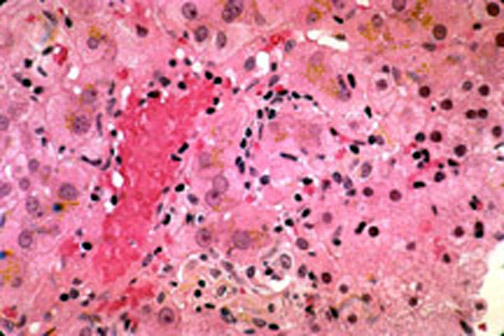 |
Fig. 8-4-7. Dilantin hepatitis.
This slide shows cytoplasmic cholestasis and sinusoidal beading of lymphocytes.
|
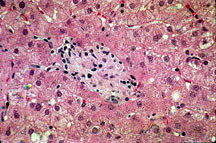 |
Fig. 8-4-8. Same case. Presence of a large Histiocytic granuloma, sharply demarcated, without necrosis.
|
|
MTHOTTREXATE |
|
Methotrexate The changes produced by this drug in the liver, in order of progressive severity, are: steatosis, ballooning degeneration, cell necrosis, nuclear changes, cholestasis, Ito cell hyperplasia, portal inflammation, progressive fibrosis, cirrhosis. Liver damage is directly related to DURATION of therapy and inversely related to the LENGTH OF INTERVALS between doses. Daily small doses are more dangerous than weekly large doses. The treatment must be monitored with repeat liver biopsies. Biochemical tests are insufficient for assessing the hepatic injury. |
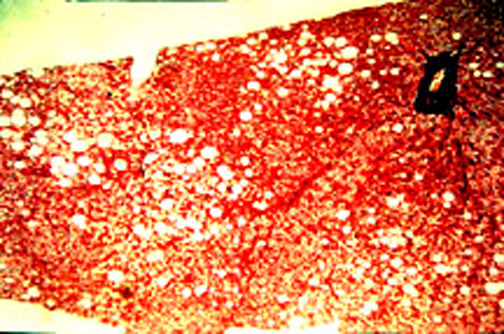 |
Fig. 8-4-9. Methotrexate hepatitis. Early lesion. In this case there is only the earliest change: focal microvesicular steatosis.
|
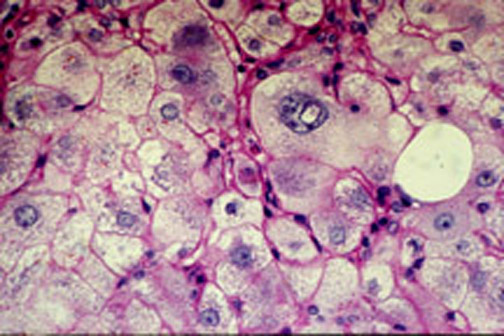 |
Fig. 8-4-10. Another case, advanced lesion.In this case the lesion is more advanced: there id ballooning degeneration, cellnecrosis, nuclear changes, fine cholestasis and beginning fibrosis,
|
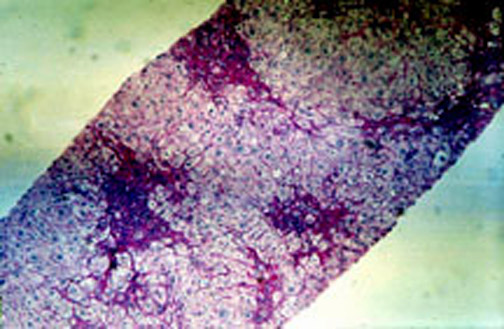 |
Fig.8-4-11.
Another case, Late lesion.
Besides the above illustrated cellular changes, in this case there is fibrosis, portal, periportal and porto-potal in some areas. |
| IV TETRACYCLINE CAUSING MICROVESICULAR STEATOSIS |
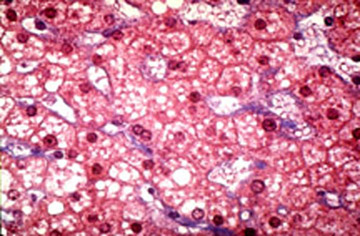 |
Fig. 8-4-12. Microvesicular steatosis, due to IV tetracyline Small fatty droplets, perinuclear. are filling the hepatocytes and imparting a foamyappearance to these cells. There is no cell necrosis and no inflammatory reaction.Microvesicular steatosis similar to that induced by IV tetracycline ocurs in acute fatty liver of pregnancy.
|
|
GRANULOMATOUS HEPATITIS |
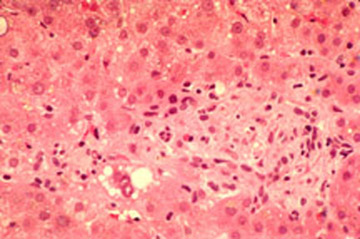 |
Fig. 8-4-13. Granulomatous hepatitis. This slide is from a patient treated with sulpha drugs. There is an intralobularhistiocytic granuloma, non- caseating.
|
|
VENO-OCCLUSIVE DISEASE |
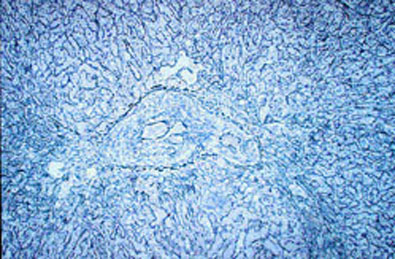 |
Fig. 8-4-14. Veno-Occlusive Disease (VOD). Obliteration of a central vein in a central vein in a case of immunosuppressive therapyfor bone marrow transplant. The obliteration occurs by endovascular fibrosis which is not theresult of an organized thrombus. The mechanism is similar to the fibrosist occurring in the ductus arteriosus immediately after birth because of reduction of the blood flow.
|