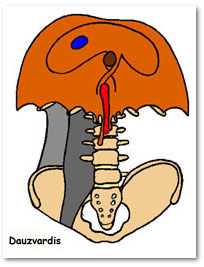
Diaphragm
Cone-shaped partition between thorax and abdomen
Chief muscle of inspiration
Pathway for spread of disease between thorax and abdomen
http://www.meddean.luc.edu/lumen/MedEd/GrossAnatomy/dissector/muscles/images/dph.jpg
Components
Musculotendinous sheet
Central tendon
Central tendon is a broad sheet of decussating tendinous fibers Pericardium is firmly attached to the upper surface of central tendon
Muscle fibers
Right and left leaflets
Two parts - crural and costal
Vertebral:crura from bodies of L1, 2 (left), L1-3(right).
Lumbar diaphragm (posterior portion), muscle fibers are long
Costal: med and lat arcuate ligs, inner aspect of lower six ribs .
Sternal: two slips from post aspect of xiphoid
Insertion: Muscle fibers insert into central tendon
Crural: From - L1,2,3 and the medial and lateral arcuate ligaments. To - Central tendon.
Function: normally it displaces abdominal contents only.
Costal: From - lower 6 ribs. To - Central tendon.
Function: normally it displaces abdominal contents and elevates and expands lower rib
cage. The extent of each depends on abdominal and thoracic compliance.
Nerve supply
Phrenic Nerve (motor) (C3, 4, 5).
Sensory: Phrenic, intercostals(6-12) and upper two lumbar N roots
Action
Inspiration and assists in raising intra-abdominal pressure
Chief muscle of inspiration
Optimal position at the beginning of inspiration is important for efficient diaphragmatic function
Radiological recognition
Actual position of the diaphragm is infered
Visualized only when inner aspect is marginated by intraperitoneal fat, fatty liver or outer aspect by lung
The left hemidiaphragmatic dome relates to the contiguous mass of the left side of heart
Defects
Triangular spaces between muscle fibers arising from sternum and those arising from 7th rib constitute weak area in the diaphragm (the foramina of Morgagni.
Deficiencies in the origin of the muscles from the posterolateral rib cage similarly creates the foramina of Bochdalek
5. Following upper abdominal surgery:
A.There is no alteration in the function of the diaphragm
in most patients
B.There is often severe impairment of diaphragm
function which can significantly impair patients with
COPD
C.Theophylline may help improve diaphragm function
a is false
Paralysis
Etiology
Interruption of phrenic nerve due to malignancy
Idiopathic
always on right
usually males
Cardiovascular surgery/Cardioplegia
Radiological findings
Elevated hemi diaphragm
Paradoxical motion (inward movement of the
abdomen ) with inspiration during inspiration and sniffing
Mediastinal swing during respiration
Pulmonary funsction
Decrease in the vital capacity and NIF
Significant change in upright versus
supine vital capacity
Symptoms
Dyspnea on effort
Dramatic orthopnea
Physical examination
Place flat portion of one hand in infraclavicular region and the other below costal margin. Note the
contribution of intercostals and diaphragm in expanding the chest. Make a similar assessment of the
other side.
Infracostal Movement:
Apply both your palms along infracostal region and note the symmetrical downward displacement of
hands with deep inspiration. There is symmetrical outward movement of epigastrium with inspiration. In
diaphragmatic paralysis there will be ipsilateral inspiratory retraction of epigastrium (Paradoxical
movement). This results in see-saw movement of epigastrium during respiration.
Tidal Percussion:
Percuss diaphragmatic position with deep inspiration and expiration and assess the depth of mobility.
Orthopnea:
Diaphragm assumes 80% function for inspiration in supine position. Hence if the diaphragm is paralysed,
significant compromise occurs and patients become very short of breath.
Impaired function due to position of diaphragm
Hyperinflation in COPD
Massive pleural effusion
Tension Pneumothorax
In these conditions the diaphragm is pushed down and is either horizontal or concave upwards. With contraction of muscles there is no significant downward movement of diaphragm and it can be paradoxical when it is concave upwards.
Diaphragm paralysis is associated with the following:
A.No change in the vital capacity or NIF, upright versus
supine
B.Abdominal paradox, inward movement of the
abdomen with inspiration
C.Recent cardiac surgery
D.Rapid development of orthopnea when becoming
supine
A is false
Eventeration
Failure of muscular development
Thin membranous sheet attached to normal muscle at points of origin
Almost exclusively on left
Roentgenologic signs similar to paralysis
Asymptomatic in adults
In neonates respiratory CV and GI distress requiring surgery
Diaphragmatic hernias
Esophageal hiatus
Mass in the posteroinferior mediastinum
Containing a fluid level
Incarceration and volvulus are the complications
Foramen of Bochdalek
80-90% occur on left side
Pleuro-peritoneal hiatus
Ipsilateral diaphragm is partly or completely obscured
multiple radiolucencies seen in hemi thorax
heart and mediastinum shifted to opposite side
ipsilateral lung compression
complete absence of intestinal gas within abdomen
Foramen of Morgagni
retrosternal or parasternal
cleft bounded by diaphragmatic muscle fibers originating from sternum medially and from the seventh costal cartilage laterally
most hernias on right
peritoneal sac present
omentum is the most common content
smooth well defined opacity in the right cardio-phrenic angle
transverse colon is situated high in the abdomen with a peak situated anteriorly and superiorly
Traumatic rupture
{kind=link}