Wednesday, December 6, 2000
9:30am – 11:30AM
CASE NO. 1
CHIEF COMPLAINT: Cough and fever for four days
HISTORY: Mr. Alcot is a 68 year old man who developed a harsh, productive cough four days prior to being seen by a physician. The sputum is thick and yellow with streaks of blood. He developed a fever, shaking, chills and malaise along with the cough. One day ago he developed pain in his right chest that intensifies with inspiration. The patient lost 15 lbs. over the past few months but claims he did not lose his appetite. "I just thought I had the flu." Past history reveals that he had a chronic smoker's cough for "10 or 15 years" which he describes as being mild, non-productive and occurring most often in the early morning. He smoked 2 packs of cigarettes per day for the past 50 years. The patient is a retired truck driver who has been treated for mild hypertension, bronchitis, appendicitis (as a young adult), hemorrhoids and a fractured femur and splenic injury. (motorcycle accident).
PHYSICAL EXAMINATION: The patient is an elderly man who appears tired haggard and underweight. His complexion is sallow. He coughs continuously. Sitting in a chair, he leans to his right side, holding his right chest with his left arm. Vital signs are as follows: blood pressure 152/90, apical heart rate 112/minute and regular, respiratory rate 24/minute and somewhat labored, temperature 102.6°F. Examination of the neck reveals a large, non-tender hard lymph node in the right supraclavicular fossa. Both lungs are resonant by percussion with one exception: the right mid-anterior and right mid-lateral lung fields are dull. Auscultation reveals bilateral diminished vesicular breath sounds. Bronchial breath sounds, rhonchi and late inspiratory crackles (are heard) in the area of the right mid-anterior and right mid-lateral lung fields. The remainder of the lung fields is clear. Percussion and auscultation of the heart reveals no significant abnormality. Examination of the fingers shows clubbing.
LABORATORY: WBC 17,000/mm3; neutrophils 70%, bands 15%, lymphocytes 15%.
COURSE OF ILLNESS: Following a chest x-ray PA view and lateral , which revealed an acute pneumonia in the right middle lobe, the patient was treated with antibiotics as an outpatient. During the 10 days of treatment the patient's fever abated and he felt somewhat better. A post-treatment (follow up) chest x-ray reveals a right hilar mass. Sputum cytology demonstrates atypical cells.
1.Identify the problems from the history.
2. Identify and explain the significance of physical findings.
3. Review the lab findings. What is your diagnosis?
- Lobar Pneumonia
- Bronchogenic Carcinoma
4. What do you understand by the terms "hospital acquired" and "community acquired " pneumonia.? Which type of pneumonia does our patient have?
Oropharyngeal colonization is different in the community and hospital setting. This makes a difference in the etiology of pneumonia. This patient has community acquired pneumonia.
5. What organisms are likely to be causing his pneumonia?
The patient has community-acquired pneumonia.
The most common organisms are
Streptococcus pneumoniae (30%)
Hemophilus influenzae (10%)
Mycoplasma pneumoniae (10%)
Chlamydia pneumoniae (8%)
influenza virus (7%)
Legionella species (3%)
In up to 40% cases, no pathogen is identified
gram negative Enterobacteriaceae (3%)
Chlamydia psittaci (1%)
Moraxella catarrhalis (0.5%)
other pathogens (8-10%)
6. List the various host factors, or conditions which predispose a patient to developing pneumonia. What host factors may have predisposed this patient to pneumonia?
Healthy adults have intact pulmonary clearance mechanisms that remove aspirated secretions.
Damaged clearance mechanisms
smoking
chronic bronchitis
asthma
viral respiratory infections
Systemic defects
malnourished persons
alcoholics
residents of nursing home
patients with heart disease
diabetes mellitus
liver disease
kidney disease
HIV infection.
Inability to mount an antibody response
lymphoma
myeloma
cancer
splenectomy
Mr. Alcot has the following predisposing factors.
He is a long time smoker and has chronic bronchitis. These conditions damage and impair the mucociliary clearing mechanism of the lung.
A bronchogenic cancer partially occluding the middle lobe bronchus prevents proper drainage of the lobe, allowing secretions to build up and inflammation to develop distal to the obstruction.
Splenectomy in this patient leads to lack of opsonizing antibody and predisposes to fulminant bacteremia with encapsulated organisms. The spleen is the principal site of clearance of pneumococci from the blood.
7. Explain the pathogenesis of pneumococcal pneumonia? What virulence factors are important? What pathologic changes are produced in the lungs because of pneumonia?
S. pneumoniae lives in the nasopharynx, and can be cultured in 5-10% healthy adults, 20-40% children. Nearly all infants are colonized at some point in the first two years of life. In epidemics involving a closed population, 5-10% of all persons carry the epidemic strain.
Aspiration of respiratory secretions containing pneumococci is generally followed by cough and epiglottic reflexes, mucociliary action and phagocytosis.
If these defenses are impaired, pneumococci multiply in alveoli.
If there is sufficient level of circulating antibody to the capsular polysaccharide, the infections is controlled. If not Serous edema fluid is poured out, which interferes with gas exchange and facilitates spread.
By the fourth day, neutrophils predominate and the alveoli consolidate.
This process usually affects a single lobe in the lung.
Bacteremia results from multiplication of the organisms.
Destruction of pneumococci occurs when anticapsular antibody is formed pneumococci are phagocytosed. Granulocytes are replaced by macrophages, and resolution of the lesion occurs.
Damage to the lung is uncommon, and recovery is associated with complete resolution of the pathologic changes.
The major virulence factor is the
pneumococcal capsule, which prevents phagocytosis by PMN’s.
Antibody to the capsule confers immunity.
Pneumolysin is toxic to pulmonary cells and causes cell lysis.
Other factors include pneumococcal protein A (Psp A), adhesins, alpha protease, and neuraminidase.
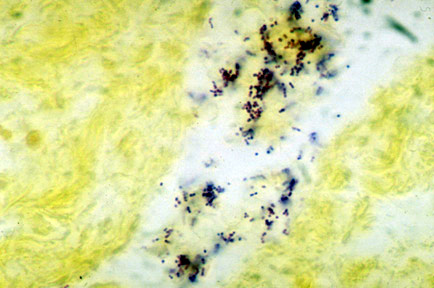
8. How is the specific diagnosis established? What is the primary disadvantage to the examination of expectorated sputum? Describe characteristic morphology/growth of S. pneumoniae.
S. pneumoniae are gram positive diplococci which produce alpha hemolytic colonies on blood agar. It is distinguished from viridans streptococcus by susceptibility to Optochin and by bile solubility.
9. What antimicrobial agents would you prescribe for this patient? Would you use or avoid penicillin, and why? What is the duration of treatment?
Penicillin has been the standard drug to treat pneumonococcal pneumonia. Procaine penicillin G, amoxicillin, cefazolin, and erythromycin are effective.
Trimethoprim-sulfamethoxazole should be avoided as up to 20% isolated from day care centers are resistant.
In penicillin – allergic patients, erythromycin is an alternative.
The emergence of penicillin resistant strains is of great concern . Where the incidence of resistance of high, Ceftriaxone or erythromycin are the agents of choice.
At LUMC, the incidence of resistance is approximately 20%.
The length of treatment will vary with the severity of illness and the presence of underlying disease.
Generally, 7-10 days of antibiotic should be sufficient.
Pneumococci are no longer detected in the sputum within several hours of the first dose of penicillin.
Dramatic symptomatic improvement in 24 hours
The lack of lung destruction and complete resolution of pathologic changes on recovery, coupled with the dramatic response to penicillin, allow for a relatively short duration of treatment.
10. What is the mechanism of pneumococcal resistance to penicillin?
Penicillin acts by binding to and blocking the action of cell membrane enzymes (PBP’s) responsible for cell wall synthesis.
Alteration of penicillin – binding proteins requires high concentrations of penicillin to saturate them, and leads to resistance.
Intermediate resistance to penicillin is defined as an MIC between 0.1 and 1 microgram. These isolates may be treated with ceftriaxone, erythromycin or increased doses of penicillin.
High-level resistance occurs when MIC is > 2 microgram. These isolates should be treated with vancomycin.
11. What are the complications of Pneumococcal pneumonia?
12. Is prevention possible?
Pneumococcal vaccine containing capsular polysaccharide from the 23 serotypes that most commonly cause infection is available.
Vaccination is recommended for individuals with chronic pulmonary or cardiovascular disease, diabetes, alcoholism, cirrhosis, chronic renal insufficiency, CSF leak and everyone above the age of 65.
In addition, immunocompromised patients with lymphoma, Hodgkin's, myeloma, organ transplantation, splenic dysfunction and HIV infection should be vaccinated.
Vaccination once in 5 years
Mr. Alcot’s enlarged supraclavicular lymph node represents a metastasis (Virchow’s node).
A 15 year old female with a history of hay fever develops fever, headache and malaise for 4 days followed by a nonproductive cough and scratchy throat. Despite chicken soup and orange juice, the cough and fever persist, and her mother drags her to your office. On examination, her temperature is 101°, pulse 90 beats/min, BP 110/70, respiratory rate 20 beats/min Physical examination is unremarkable except for scattered rales over the left lower lung, and small bullae in her left tympanic membrane. Chest x-ray reveals a patchy left lower lobe infiltrate. At your request, she makes a heroic effort but is unable to produce sputum
1. What is the type of pneumonia this patient is likely to have?
Atypical pneumonia.
2. What is "atypical pneumonia"?
The term "atypical pneumonia" is applied to non-lobar patchy or interstitial infiltrates on chest x-ray where the causative organism is not identified on gram stain or culture of sputum.
Often they are not toxic, do not have shivers and do not seek medical attention. "Walking Pneumonia"
3. What is the differential diagnosis of atypical pneumonia?
The pathogens causing atypical pneumonia include
Mycoplasma pneumoniae
Chlamydia psittaci
Chlamydia pneumoniae
Coxiella burnetii
Francisella tularensis
Legionella pneumophila
viruses including influenza A and B, parainfluenza, adenovirus and respiratory syncytial virus.
4. What is the most likely organism in this patient and why?
Mycoplasma pneumoniae
Many of the agents listed above could be responsible for this patient’s pneumonia. Features pointing to Mycoplasma include her
age (commonly between 5-15 years)
scratchy throat (tracheitis) and
bullae in tympanic membrane (bullous myringitis)
5. Describe Mycoplasma pneumoniae.
Mycoplasma pneumoniae is one of the smallest free-living microorganisms.
It lacks a cell wall, and hence stains poorly on usual bacterial stains.
It grows aerobically and produces tiny colonies on special agar that have an "inverted fried egg" appearance.
Hemadsorption of red blood cells on the surface of agar plates is a feature of Mycoplasma pneumoniae.
6. What is the pathogenesis of infection produced by these agents? What pathologic changes are produced in the lungs?
Mycoplasma pneumoniae attaches to the cilia and microvilli of cells lining the bronchial epithelium.
Attachment is mediated by a surface adhesion, the P1 protein, which binds to oligosaccharides containing sialic acid in the bronchial epithelial cells.
Ciliary action is stopped followed by loss of cilia and desquamation of epithelial cells into the lumen.
Oligosaccharide receptors (1-F1) are not found in non-ciliated cells or mucus; hence mycoplasma pneumoniae does not for some of the damage produced.
Sloughing of cells into the lumen is responsible or the cough that defines the clinical presentation.
The inflammation conspicuously involves the interstitial space or alveolar wall with mono-nuclear cells.
The inflammatory process involves the trachea, bronchioles, and peribronchial tissues.
The lumen is filled with purulent exudate containing polymorphonuclear leukocytes.
Bronchial and bronchiolar walls are infiltrated with monocytes and plasma cells.
There is widening of peribronchial septae and hyperplasia of type II pneumocytes.
Organisms are shed in respiratory secretions for 2-8 days after onset of symptoms, and shedding can continue for as long as 14 weeks after infection.
Other pathogens producing atypical pneumonia produce similar pathologic changes.
7. How does immunity to Mycoplasma pneumonias develop ? Is reinfection possible?
Local and systemic specific immune responses occur.
IgA antibody wanes 2-4 weeks after onset of infection.
Complement-fixing serum antibodies peak at 2-4 weeks and disappear in 6 to 12 months.
Nonspecific immune response to the outer membrane also develop e.g., cold hemagglutinins (IgM antibodies that react with I antigen of human RBC’s).
Immune mediated mechanisms play a role in M. pneumoniae infection.
Reinfections is associated with quicker development of inflammatory changes in experimental animals.
High levels of IgG immune complex are found in the acute phase of illness and correlate with degree of pulmonary involvement.
M. pneumonia can stimulate B and T lymphocyte mitogenic activity.
Immunity to M. pneumoniae is not complete, and re-infection is common.
Clinical disease is more severe in older children, suggesting that many clinical manifestations are due to cellular immune responses.
8. How is the diagnosis established in atypical pneumonia?
Definitive diagnosis is made by isolation of the organism or demonstration of an antibody response.
Isolation of M. pneumoniae on SP-4 medium takes 2-3 weeks and is too expensive and time consuming.
Detection of M. pneumoniae antigens or nucleotide sequences in clinical specimens by enzyme immunoassay or per DNA hybridization is under development.
The compliment fixation test detects specific antibody and is commonly used. Antibody rises 7-9 days after infection, peaks at 3-4 weeks and lasts for 6-12 months. A four-fold rise or decline in titer is necessary for diagnosis.
Two thirds of patients with symptomatic M. pneumoniae pneumonia will develop high titers of cold agglutinins. These are not specific and are seen in other viral infections (adenovirus, EBV). This test is simple and can be performed at the bedside.
New assays include indirect immunofluorescence and ELISA and detect IgM as well as IgG. An ELISA using adhesion PI protein is being developed.
Antigen detection and culture of sputum for specific pathogens helps establish the diagnosis in other cases of atypical pneumonia. Serology is useful but acute convalescent titers are needed.
9. What antimicrobial agent(s) would you use ?
Erythromycin and tetracycline are equally effective in treatment of M. pneumoniae infection.
They shorten the course of infection but do not eliminate the carrier state.
Clarithromycin and azithromycin are also effective but much more expensive.
Quinolones such as ciprofloxacin have in vitro efficacy against mycoplasma, but are expensive and contra-indicated in children.
Since mycoplasmas lack a cell wall, beta-lactam antibiotics are ineffective for treatment.
Therapy is generally continued for 2-3 weeks, as relapses can occur in up to 10% cases.
10. You start the patient on Erythromycin. If he is taking antihistamines, what drug interaction might occur?
Elevations of terfenadine and astemizole serum concentrations have been associated with concomitant use of erythromycin (and clarithromycin).
Erythromycin interferes with the hepatic metabolism of these drugs through the cytochrome P-450 system.
Erythromycin metabolites form inactive complexes with cytochrome P-450 enzymes.
Elevated levels of these antihistamines have led to serious ventricular arrhythmias.
CASE NO. 3
A 35 year alcoholic male with a history of seizures is admitted with a three week history of fever, generalized weakness, poor appetite, and cough productive of green, foul - smelling sputum. On physical examination, the temperature is 100.3 degrees P. pulse is 96 beats per minute, respiratory rate is 20 breaths per minute, and BP is 120/80 mm. There are many missing teeth with gingivitis and dental caries. He has rales and decreased breath sounds over the right base. Chest x-ray shows consolidation in the superior segment of the right lower lobe.
1. What type of infection is suggested by his foul smelling sputum?
Anaerobic infection.
2. What organisms could be responsible for this patient's pneumonia?
Many of the infections are polymicrobial.
Anaerobic bacteria are found in 60% to 85% of the cases.
50% of patients have only anaerobic organisms, while the other 50% have a combination of aerobic and anaerobic organisms with and anaerobic predominance.
Anaerobes that are frequently found include:
- Peptostreptococcus sp.
- Bacteroides sp. (B. melanogenicus, B. intermedius)
- Fusobacterium sp.
Aerobes that my be found in predominant anaerobic infection include:
- Microaerophilic streptococci
- Eikenella corrodens
- Pseudomonas aeruginosa
- Staphylococcus aureus
- Enterobacteriaceae
3. Does a normal person aspirate?
50% of healthy persons aspirate during sleep, usually goes unrecognized, and has few sequelae.
4. What then determines who gets infection?
The frequency, volume, and character of the aspirated material will determine whether or not a pulmonary infection will develop.
5. What are the other predisposing factors for aspiration? What factor/s predisposed this patient to aspirate?
Factors associated with increased frequency of aspiration include.
His alcoholism and seizures probably are the predisposing factors for him. Gingivitis and caries provided a bigger bacterial inoculum for aspiration.
6. Describe the pathogenesis of this pneumonia.
7. What are the common sites for aspiration lung abscess and why ?
The superior segments of RLL, LLL and axillary subsegments of anterior and posterior segments of RUL are
common sites for aspiration and will account for 85% of all Lung abscesses.
Gravitational forces determine the site of aspiration. Position of the patient at the time of aspiration determines
the segment the aspiration is most likely to occur.
8. What is the normal clinical picture of lung abscess?
Does this patient fit that clinical picture?
Most of the patients present with sub acute onset of illness and do not seek medical attention for three to four weeks since the onset of illness.
Patients complain of cough, low grade fever, anorexia and weight loss of few weeks duration .
Patients often have cough with large amounts of foul smelling sputum.
Lack of foul smell does not exclude lung abscess, as 50% of anaerobic infections do not produce a foul smell.
Our patient has the typical clinical picture.
9. Are there other routes besides aspiration by which anaerobes can reach lungs?
Less common mechanisms by which anaerobic bacteria reach the lung include:
- Transdiaphragmatic spread from subphrenic collections,
- Hematogenous spread from septic thrombophlebitis, and
- Tissue necrosis caused by pulmonary infarction, bronchiectasis, and bronchogenic carcinoma may serve as a nidus for anaerobic infection.
10. What complications are associated with this infection?
If aspiration pneumonia goes untreated, progressive tissue necrosis may ensue. This results in
- Abscess formation
- Necrotizing pneumonia
- Bronchopleural fistula
- Empyema
11. How would you treat this patient?
Metronidazole should not be used as a single agent (because of its high failure rate). If metronidazole is used, penicillin also should be used to cover aerobic and microaerophilic streptococci.
Duration of therapy will depend on radiographic clearance, and may range as long as 2-4 months.
Postural drainage is an important component of therapy.
Rarely surgical therapy (lobectomy) may be required in non-resolving cases, and in patients with hemorrhage.
If an empyema develops treat with chest tube drainage in addition to antibiotic therapy.
12. What organisms might be the cause of a hospital acquired aspiration pneumonia?
Patients with nosocomial aspiration pneumonia are more likely to have a mixed aerobic-anaerobic infection, in which the aerobic component (gram-negative bacilli) predominates.
Aerobic organisms:
- Klebsiella
- Enterobacter
- Serratia
- E. coli
- Pseudomonas aeruginosa
- Staphylococcus aureus
Anaerobic organisms:
- Peptostreptococcus sp.
- Bacteroides sp. (B. melanogenicus, B. intermedius)
- Fusobacterium sp.
Antibiotics
{kind=link}