THURSDAY, NOVEMBER 16, 2000
9:30AM – 11:30AM
CASE HISTORY 1
05/09/1990: The patient, a 16 year old female was well until 2 days prior to admission when she had a fever to 39.9°C and vomiting. On the morning of admission, she had loose stools, continued fever, and vomiting. She was seen by her local pediatrician who noted that she was hypotensive (BP 76/48 mmHg) with a heart rate of 120 beats/min and a temperature of 38°C. She had an erythematous rash, which was most prominent on her trunk. Cultures were obtained. The patient was given intravenous fluids and IV antibiotics and transported to the hospital, where she was admitted into the Pediatric Intensive Care Unit.
Laboratory studies indicated elevated liver enzymes, increased creatinine and blood urea nitrogen, and WBC count of 14,100 mm3 with 78% neutrophils and 18% band forms. The patient had begun her menstrual period 4 days before she became ill.
QUESTIONS
1. Does this patient have infection? Is it bacterial or Viral? What evidence do you have?
Patient probably has bacterial infection. Fever is nonspecific
but an important manifestation of infection. Her WBC count shows leucocytosis,
and shift to left which supports a response to bacterial infection. WBC
features of bacterial infection are:
2. What are the potential sites for infection in this patient as judged from the clinical story?
3. What additional history would you like to have? How can infection be linked to her periods?
She must have used Tampons for her periods. Infection can be associated with Tampon use. Did she use tampons?
4.. Yes she did use tampons for her periods. Her blood pressure is low indicating that she may be in shock. What are the types of shock you can encounter with infection?
5. Which shock do you think the patient is in and why did you come to that conclusion?
Toxic shock: She has the classical constellation of toxic shock syndrome characterized by
6. What type of infections can lead to Toxic shock syndrome?
Toxic shock syndrome is caused by strains of
7. What cultures would you consider obtaining form this patient
8. The vaginal culture was positive for many catalase positive, Gram positive cocci. What organism do you expect this to be?
The organism is most probably Staphylococcus aureus.
9. What is the normal flora of Vagina? Since S. aureus is one of the normal flora of vagina how can you attribute significance to the culture results?
The finding of many S. aureus in the vaginal tract is supportive but does not prove the diagnosis of toxic shock syndrome.
S. aureus can be normal vaginal flora in 8-10% of females, although heavy vaginal growth of S. aureus is unusual.
10. What virulence factor does this organism produce which is believed to be responsible for the signs and symptoms in this patient? What is the pathophysiology of Toxic shock syndrome? How do these toxins lead to the clinical manifestations?
TSST-1 is a true exotoxin because it is secreted during cell growth rather than after cell lysis.
This toxin is a super antigen which activates T cells by binding antigen-presenting cells to the V$ chains of the T-cell receptor.
Super antigens can activate 5-25 % of the total T-cell population rather that 1-2% activated by the more physiological mechanism of processed antigen causing excessive release of cytokines (IL-2, TNF), that leads to many signs and symptoms of the illness.
11. What do you need to prove that the staphylococcus that has been cultured from vagina is responsible for the toxic shock in this patient?
In order to prove this isolate is the etiologic agent of toxic shock syndrome, it should be demonstrated that the isolate produced Toxic Shock Syndrome Toxin-1 (TSST-1).
12. This patient's isolate was shown to produce this virulence factor. This toxin in animal models has been shown to reproduce some of the same clinical characteristics of this disease as seen in humans. What is the significance of tampon use in this patient?
One of the key observations in the initial epidemic of TSS was that the disease was most severe in women who used super absorbent tampons.
It is known that TSST-1 is produced under conditions of low magnesium ion concentration.
It is speculated that the tampons act to absorb various ions including magnesium, providing optimal conditions for production of TSST-1.
13. When the association between super absorbent tampons and TSS became clear, this product was withdrawn from the US marketplace. With this suspension in sales came a marked decrease in the number of cases of TSS reported in menstruating women. Does that mean we do not encounter Toxic shock syndrome anymore?
No.
These strains are found in surgically related infections and at other body sites.
A similar type of illness is also caused by Streptococcus pyogenes, which produces streptococcal pyrogenic exotoxins SPE A, B. or C.
14. What is our therapeutic strategy?
Therapy consists of fluid and electrolyte replacement and identification and drainage of any focally infected site, such as an abscess. Antibiotic therapy should be based on the susceptibility pattern of the isolate. The following antibiotics can be used
Penicillin
Mthicillin resistant Staph aureus
15. What are the clinical presentations of S. aureus infection?
Both Staphylococcus aureus and Streptococcus pyogenes (group A strep) have many enzymes which act as virulence factors allowing these bacteria to invade tissue from patients with normal immunity and spread from infection at a local site to the bloodstream.
CASE HISTORY 2
A 6 year old female awakened with pain and swelling in the right ankle. Four weeks ago she had a febrile illness with a sore throat and headache and was treated with amoxicillin. On admission, she had a warm, swollen right ankle and a new systolic heart murmur thought to be consistent with mitral regurgitation.
QUESTIONS
Casse 2
1. The patient previously had a sore throat and although we do not have culture results from that illness, what pathogen would likely have grown from her throat culture?
Common causes for Pharyngitis are:
Throat culture four weeks after Pharyngitis and following Amoxacillin is most likely to be negative.
It should be noted that viral pharyngitis occurs at least as frequently as strep pharyngitis, therefore, a rapid test antigen screen (45 minutes) for Streptococcus pyogenes or a culture (48 hours) is used to establish the diagnosis (catalase negative colonies which are beta hemolytic).
2. What is the relationship between her pharyngitis and the subsequent development of joint problem? What is your diagnosis and why?
We need to consider
Rheumatic fever is a reasonable choice because of
Rheumatic fever occurs in about 3% of times following Streptococcal pharyngitis.
3. What is Rheumatic fever?
Rheumatic fever is a non-suppurative sequela of Streptococcus pyogenes infections.
It occurs approximately 3 weeks after streptococcal pharyngitis.
By the time the symptoms are apparent, the throat culture is negative. A recent history of streptococcal pharyngitis supports the diagnosis of rheumatic fever.
Rheumatic fever is characterized by
Migratory ployarthritis
Carditis
Sub Q nodules
Erythema marginatum
Sydenham Chorea
4. What hemolysins does this organism produce which help to identify infection with this organism?
Colonies of Streptococcus pyogenes are beta hemolytic due to two distinct hemolysins: streptolysin S and streptolysin O.
The beta hemolytic streptococci are classified into Lancefield groups based on unique carbohydrate antigens in their cell wall. Streptococcus pyogenes is designated as Lancefield group A.
Unlike streptolysin S. streptolysin O is oxygen labile. Throat cultures must be incubated anaerobically or the blood agar plates must be stabbed to demonstrate the potent hemolysin, streptolysin O (Cytotoxin, lyses RBC's and WBC's).
5. In the absence of positive culture what other evidence can you seek for recent prior Streptococcus pyogenes infection?
Patients with RF will frequently mount (80%) a humoral immune response to streptolysin O.
The test used to measure antibodies against this hemolysin is called an ASO (anti-streptolysin O) titer. An elevated ASO titer in individuals with appropriate clinical symptoms supports the diagnosis of RF, when culture results are negative.
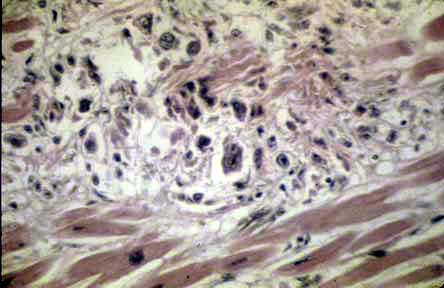
6.What is the pathogenesis of rheumatic fever ?
M protein is an important virulence factor found in the cell wall (Pili) of Streptococcus pyogenes.
M protein has been found to be antiphagocytic and it also has epitopes which are antigenically similar to one found in the cardiac myosin and sarcolemmal membrane proteins.
Acute RF is thought to be an auto-immune disease. Antibodies directed against M protein cross-react with cardiac tissue. These antibodies bind to the cross-reactive antigens in muscle and damage the muscle tissue. Other group A strep antigens may also cross-react with other cardiac antigens causing damage to the heart valves.
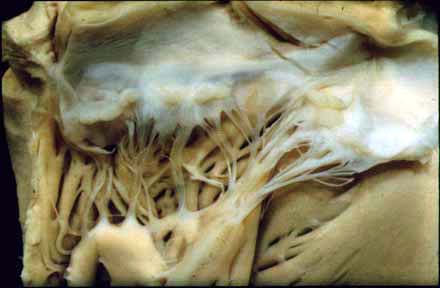
Acute : Causes Pancarditis (Pericardium, Myocardium and endocardium)
Chronic: Progressive valvular fibrosis with thickening and sclerosis of valves, adhesion of commisures, thickening, shortening and adhesions of chordee, calcification.
7. What are the other virulence factors of Streptococcus pyogenes ?
Additional virulence factors of S. pyogenes include These enzymes help spread infection further into tissue.
Hyaluronidase
DNase
Streptokinase : Lyses fibrin
clots
Erythrogenic toxin.
8. What are the clinical presentations of group A streptococcal infection?
Pharyngitis: Sorethroat, fever, cervical lymphadenopathy, swollen red tonsils with white or yellow patches
Rheumatic fever: Auto-immune process. Systemic inflammation affecting Heart, Joints and Skin.
Acute Glomerulonephritis: Auto-immune process.
Toxic shock syndrome: Pyrogenic exotoxins A,B or C. Stimulates T cells to release of Cytokines. Shock and failure of multiple organs. Superantigens
Scarlet fever is a manifestation of group A streptococcal pharyngitis in which the infecting strain produces a specific virulence factor called erythrogenic toxin, which is coded for by a phage.
Production of this toxin is manifested clinically by the appearance of a scarlatinal (bright red) rash beginning on the chest and spreading to the trunk and neck, then to the extremities. The rash is not seen on the face, or the palms or soles.
A "strawberry" tongue is frequently seen with this disease as well.
Rheumatic fever can be a post-streptococcal sequela of scarlet fever just as it may be follow strep throat caused by strains which do not produce erythrogenic toxin.
Necrotizing Fascitis: Bacterial infection of fibrous tissue thatt covers the body beneath the skin. "Flesh eating bacteria" . Significant mortality.
9. How would you treat this infection?
Penicillin for 10 days to prevent recurrence or complications
Symtomatic therapy (Tylenol, Fluids and electrolytes)
Complications ( Acute glomerulonephritis, Carditis etc)
Surgical debridement: in Necrotizing fascitis
CASE HISTORY 3
A 39 year old black female was admitted with low grade fevers, weight loss, and malaise which has been ongoing for three weeks. Her past medical history is significant for chronic renal failure secondary to postpartum complications. She has an A-V fistula in her right arm through which she receives her weekly dialysis. Blood cultures were drawn over the first 24 hr of her admission. Her physical exam revealed a grade III/VI diastolic murmur, which was not present on previous exams. Within 36 hr. the aerobic and anaerobic bottles of all three sets of blood cultures turned positive. The Gram stain of the blood culture was read as Gram positive cocci in pairs and short chains. The patient was empirically treated with ampicillin and gentamicin, but she remained culture positive. Vancomycin was added to her regimen, but she did not improve.
Case 3
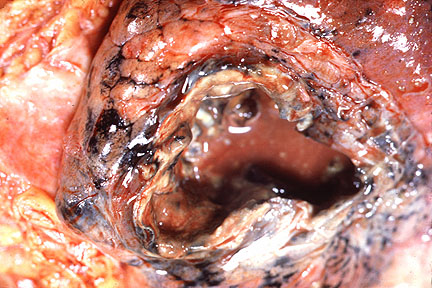
1. What infectious disease does this woman have?
She has infective endocarditis
2. What is the pathogenesis of this disease?
Normal intact endothelium resists implantation by organisms. Very virulanr pathogens may be able to cause endovascular infection. Acute infective endocarditis.
Sub acute infective endocarditis: If there is damaged valves the organisms can implant on them. Endothelial injury inflicted by the organisms release tissue factors to activate platelets and fibrin-platelet vegetaions ( clot ) forms. These start off as non-bacterial thrombotic endocarditis (NBTE). Organisms of low virulence colonize these NBTE and cause endovascular infection.
3. What signs and symptoms would you look for to verify your diagnosis?
The manifestations of infective endocarditis are protean since any organ can be involved.
Infective: Fever, Weight loss, anorexia, malaise, splenomegaly, leucocytosis
Vegetations: New murmurs, destruction of valve leading to insufficiency followed by hear failure
Embolic:
Janeway lesions (erythematous macules and papules on the palms and sole)
Osler nodes (tender raised erythematous lesions on the finger and toe pads )
Splinter hemorrhage in the nail beds
Roth spots (Petechiae in retina with white centers)
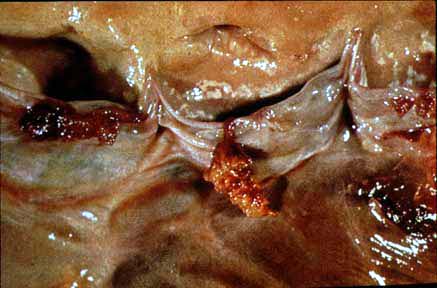
4. How would you confirm the presence of vegetations on heart valves?
An echocardiogram revealed vegetations on her aortic valve.
5. The microbiology lab reports that colonies growing on a blood agar plate are catalase negative, nonhemolytic, and stain as Gram positive cocci in chains. The colonies are bile esculin positive and PYR positive. Based on the laboratory data, which microorganism is the most likely pathogen?
The Gram stain is suggestive of a streptococcus since cocci in chains were observed.
This is verified by the negative catalase which separates the streptococci from the staphylococci.
Additional biochemical reactions of a positive bile esculin hydrolysis and PYR (pyrrolidonyl-beta-naphthyl amidase) hydrolysis are indicative of an enterococcus.
The species cannot be given based on this data. A more complete battery of biochemical testing is required to further identify which species of enterococcus was isolated.
E. faecalis is the most common species in clinical infections (85%); E. faecium is second (12%), the remaining isolates are a variety of Enterococcus species.
6. Why is this patient failing to improve on her antibiotics?
Because this organism is not susceptible to vancomycin and ampicillin, there is no adequate antibiotic therapy reaching the infection.
The organism is labeled a VRE (vancomycin resistant enterococcus).
Most likely the organism is E. faecium, which is intrinsically resistant to ampicillin and has acquired a gene to change its cell wall composition so that vancomycin can not disrupt cell wall synthesis and inhibit the growth of the bacteria.
In addition the orgnims are inside avascular vegetations, Antibiotis and Phagocytes do not have easy access. They are also in lower metabloic state.
7. What predisposed this patient to acquiring an infection with this bacterium?
The enterococci also require a breakdown of host's defenses or mucosal barriers to cause infection.
Her an A-V fistula broke down the barrier of the skin and mucous membranes and serves as a conduit for microorganisms to travel from the superficial sites into the bloodstream.
The enterococci do not have M protein, hemolysins, or toxins which act as virulence factors for the beta hemolytic streptococci.
8.What other infections are commonly caused by this group of organisms?
Usually enterococci are associated with urinary tract infections and mixed bacterial wound infections, such as decubiti. They cause sepsis and rarely meningitis.
The enterococci are normal flora of the gastrointestinal tract and are present in the gastrointestinal tract of animals and on plants. They lack the virulence factors of the staphylococci and beta hemolytic streptococci, but are significant pathogens because of their intrinsic antimicrobial resistance.
9.What infection control precautions must be taken for this patient?
Any patient whose cultures have VRE must be placed on barrier precautions, which entails gloves and gown for anyone handling the patient or objects in their environment.
A mask is not required.
When a patient has VRE, most likely they are carrying the organism in their GI tract. Items in their room readily become colonized so that VRE can be isolated from bed rails, call buttons, etc.
Hand washing is an important means by which the transmission of VRE can be reduced.
CASE HISTORY 4
A 14 month old boy was referred from another hospital for an infected ventriculo-peritoneal shunt. The baby was born prematurely and had meningomyelocele and hydrocephalus. He underwent surgery for his first shunt when he was 7 weeks old. One week prior to transfer, he was admitted to the hospital for fever. Needle aspiration of the shunt revealed a cloudy fluid which had Gram positive cocci in clusters seen on Gram stain.
QUESTIONS
Cae 4
1. What is meningomyelocele?
A form of neural tube defect.
2. What is Hydrocephalus?
Hydrocephalus is a condition in which the primary characteristic is excessive accumulation of
CSF in the brain. The excessive
accumulation of CSF results in an abnormal dilation of
ventricles with potentially harmful pressure on the tissues of the brain.
3. What is the purpose of ventriculo-peritoneal shunt?
Hydrocephalus is most often treated with the surgical placement of a shunt system. This system diverts the flow of CSF from a site within the central nervous system to another area of the body where it can be absorbed as part of the circulatory process. A shunt is a flexible but study silastic tube
4.What is the most likely pathogen to be recovered from his fluid culture?
Staphylococcus aureus, or a coagulase negative Staphylococcus species, possible S. epidermidis.
5. What kind of pathogen is S. epidermidis ?
Opportunistic pathogen.
6.What virulence factors does Staphylococcus epidermidis possess which allows it to be an opportunistic pathogen?
S. epidermidis, require a breakdown of the host's skin or mucosal barriers to cause infection.
The introduction of central lines, venous catheters, or prosthetic devices provide an entrance route to the body for this organism that does not produce the virulence factors that more pathogenic organisms do.
Once the barrier has been compromised, S. epidermidis may produce "slime", a biofilm that aids in the adherence of the bacteria to the synthetic surface of the device and protects the bacteria from phagocytosis and antimicrobials.
7. What is the most appropriate management for line infections with S. epidermidis?
Antimicrobial therapy may eliminate the organisms from the blood stream.
But persistent bacteremia indicates that the catheter must be removed for eradication of the infection.
Coagulase negative staphylococci are usually resistant to oxacillin, nafcillin, and methicillin. If the isolate is methicillin resistant, treatment with the first generation cephalosporins is not effective. Vancomycin is usually the drug of choice for methicillin resistant staph infections.
8. Where are these organisms normally found in nature and how do they gain access to the bloodstream?
S. epidermidis and other coagulase negative species of staphylococci are normal commensals of the skin, anterior nares, and external ears in humans and animals.
These organisms may contaminate prosthetic devices
(valves, shunts,
joint replacements) during implantation or post-surgical manipulation.
Neonates and
neutropenic patients are particularly at risk.
Because coagulase negative staphylococci are present on the skin, identification of staphylococci in blood cultures may represent either contamination or a clinically significant finding. Distinguishing between the two is often difficult.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}