Questions and Answers
1. Develop a limited differential diagnosis (given the data in this case-causes of chest pain with higher probability than others).
Acute Myocardial Infarction
Esophageal Disease (Spasm/GERD)
2. What is your diagnosis? Why? List and explain specific data from the history and physical exam which support this diagnosis. Explain why other diagnoses are less probable. Can the patient have two diseases, (i.e. AMI and GERD) simultaneously?
The nature of the pain, associated symptoms and signs, risk factors and past medical
history support the diagnosis of Acute Myocardial Infarction (AMI)
The chest x-ray is normal speaking against pneumonia, pneumothorax and dissecting aorta (wide mediastinum).
WHO definition for Acute Myocardial Infarction
Characteristic history of pain of Acute MI is:
He also has symptoms suggestive of GERD. Most likely he may have both problems.
3. We are satisfied that he has history of ischemic type discomfort. Let us see whether he has Cardiac markers of injury. What enzymes, if any, would you order to assist in making the diagnosis? Compare and contrast the enzyme patterns if the pathologic process was of 3 hours duration, or 24 hours duration, or 72 hours duration? You should be able to explain the various enzymes which might be elevated during the course of the infarction.
The total leukocyte count is slightly elevated with a neutrophilia. This non-specific change is compatible with necrosis of the myocardium. The remaining lab data is normal.
The classic patterns enzymes may not be elevated very early in the course of the AMI. Therefore, you should not depend on one set of enzyme determinations but must order a sequence of test over several days. The initial enzyme determination in the ER may be normal.
The total CK will begin to rise 4-6 hours after the onset of the infarct and reach a peak levels within 24 hours.
The CK-MB level rises within the same time frame and disappears in about 72 hours and gradually disappear over 7-4 days post MI.
The levels of enzymes LDH-1 and LDH-2 "flip" or reverse in AMI. Normally, the LDH level is less than the LDH-2 level. AST(SGOT) levels rise within the first 24 hours and disappear in 3-4 days.
AST and CK-MM, are not specific for myocardium. You should understand that the enzyme levels will vary depending on the amount of time between the onset of the infarct and when the test is performed.
Current markers used in clinical practice (2000)
| < 4hours | 24 hours | 72 hours | ||
| CK | Lack specificity and sensitivity | 6-8 hours | Peak increase | Normal |
| CK-MB | Less specific (skeletal injury, Hypothyroidism) | 6-8 hours | Peak increase | Normal |
| Troponin I and T | Specific Cardiac injury | 6-8 hours | Peak increase | Remains elevated (5-9 days) |
| Myoglobin | Not Cardiac specific | 2-4
hours (peak 8-12 hrs) |
Normal |
Non specific markers not that useful
| < 4hours | 24 hours | 72 hours | ||
| WBC | Non-specific | Normal | Increased | Normal |
| AST(SGOT) | Non-specific | Normal | Increased | Normal |
| LDH | LDH-1 and LDH-2 "flip" | Normal | Increased | Returns to baseline in 8-12 days |
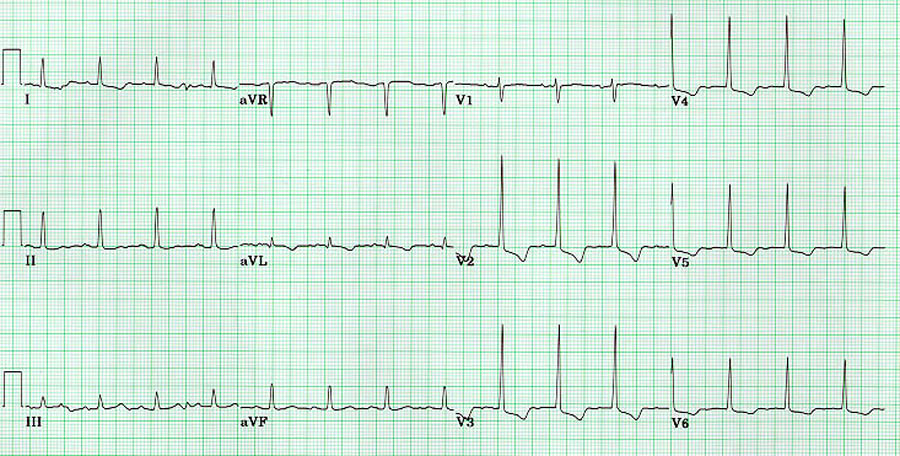
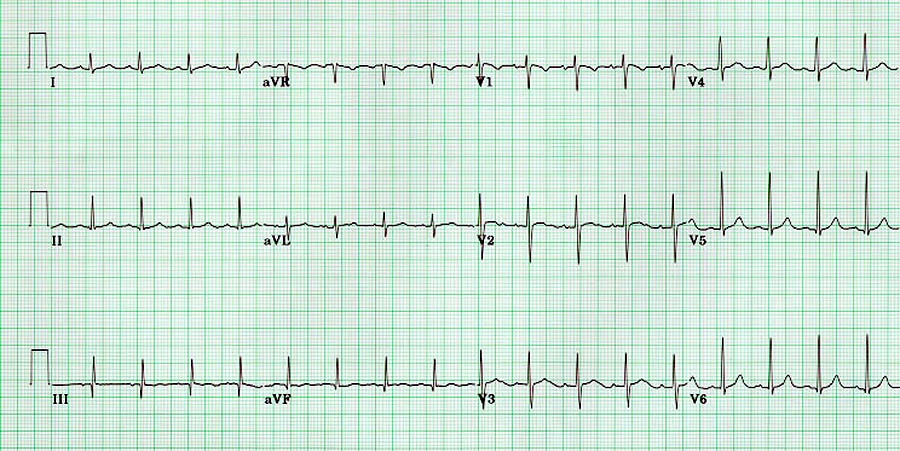
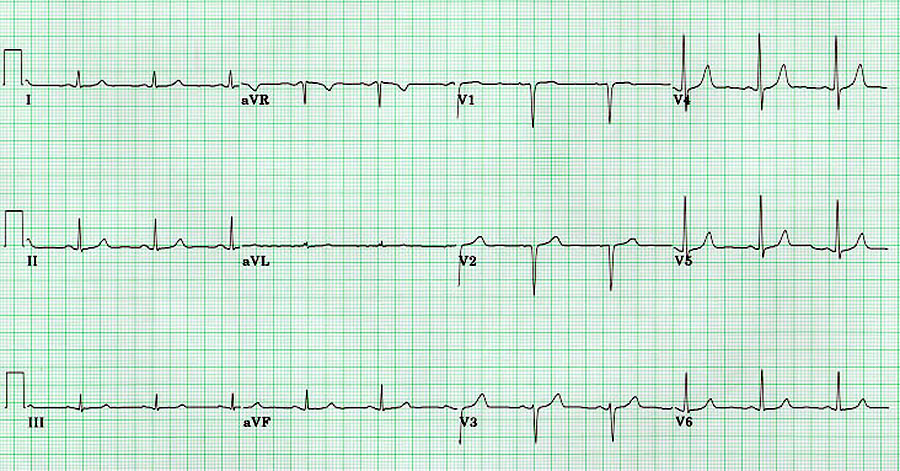
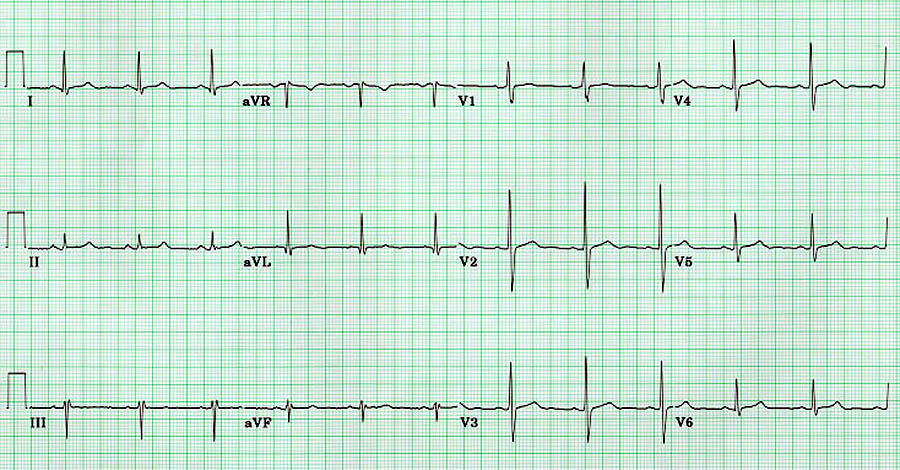
4. Next we need to determine whether he has EKG evidence for Myocardial injury/infarction. Two electrocardiograms are attached. (A) was performed when Mr. Solomon applied for an insurance policy at age 42. (B) was performed in Loyola's emergency room. Determine the rate, rhythm and axis for both ECG's. Identify any abnormality, correlating any changes with the mechanism and location of the pathologic process.
Electrocardiogram (A): Rate 70BPM, rhythm is normal sinus, axis is � 20. Normal ECG.
Electrocardiogram (B): Rate ~70BPM, rhythm is normal sinus, axis is normal.
5. What are the EKG changes of acute myocardial infarction and explain the genesis of each.
Ischemia and infarction -
Generally ischemia results in ST segment depression and more severe injury results in ST segment elevation. However, elevation and depression can actually co-exist in the same EKG depending on the position of the recording lead. There is no easy or simple explanation for the EKG changes with either of these pathologies.
It is believed that with more severe myocardial injury, intracellular potassium leaks out of damaged cells and makes the resting membrane potential more positive. As a result, current of injury flows from damaged cells to normal cells during the diastolic period (T-QRS segment). This shifts the baseline of the EKG down, giving the impression that the ST segment is elevated.
New Q waves: From the absence of depolarization current in the dead tissue and receding currents from opposite side of Heart.
R wave progression: Alterations
High probability for infarction
Normal or nonspecific ECG does not rule out acute MI. Only about half the patients will have diagnostic changes on their initial EKG.
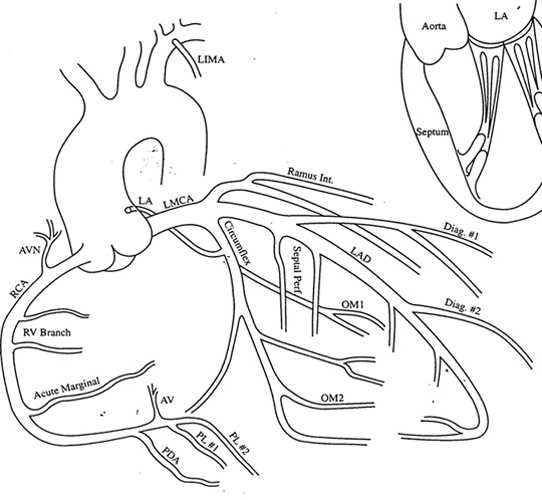
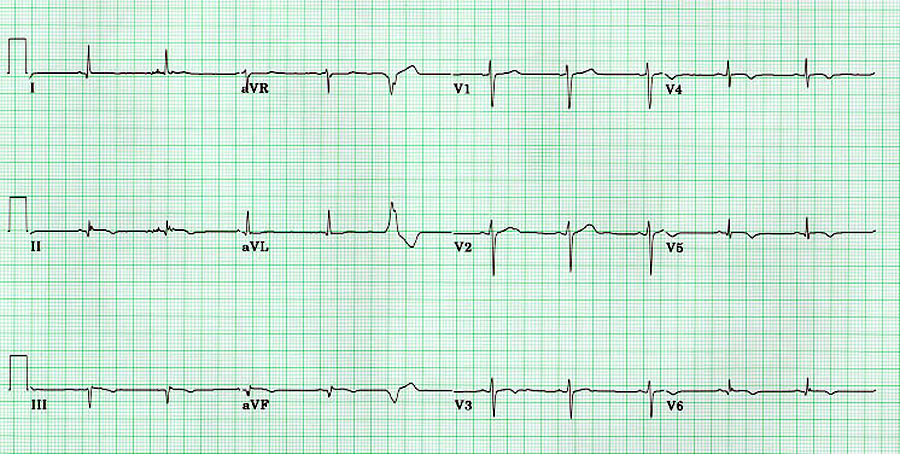
6. Correlate the site of infarction to coronary circulation
Location of Infarction/ occlusion of branch of coronary artery
| Inferior wall | II, III, AVF | RCA (if right dominant) or extension of circumflex artery (if left dominant) |
| Lateral wall | I, AVL, V4-6 | Diagonal branch of LAD or marginal branch of circumflex artery |
| Antero-septal | V1-3 | Very proximal LAD |
| Antero-lateral: | V1-6 | Proximal LAD |
| Posterior wall | R/S ratio >1 in V1 and V2. Upright T wave in V1-V2. |
Distal circumflex or distal coronary artery |
7. Describe the natural evolution of ECG changes following acute myocardial infarction.
Evolution of EKG changes over time in Acute Myocardial Infarction
| In the first few hours | Normal R waves | ST elevation | Peaked T wave | |
| Within 24 hours | Beginning of Q wave | R wave loss | ST beginning to return to baseline | T wave inversion |
| 24-48 hours | Deepening Q wave | R wave loss | ST segment returning to baseline | Continued T wave inversion. |
| After 48-72 hours | Deep Q waves | No R waves | ST usually back to baseline | |
| After several weeks | Deep Q waves | Small R wave may return | ST back to normal | |
From this information you should understand the need for obtaining sequential cardiac enzymes and EKG and learn to interpret them based on the latency between onset of pain and the time of evaluation.
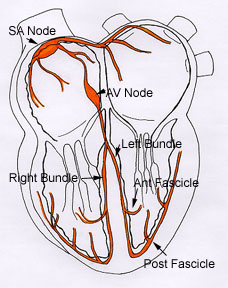
8. Correlate conduction system defects with coronary circulation
| SA Node | RCA and Left circumflex | Pacemaker of Heart |
| AV Node | RCA and LAD | |
| AV bundle | RCA and LAD | |
| Left bundle | LAD and RCA | Conduction blocks alter the changes of MI and you should be aware of it. |
| Right bundle | RCA and LAD |
You can see that the conduction system gets blood supply from both RCA and LCA.
9. Based on the catheterization, explain the probable mechanisms for Mr. Solomon's chest pain during the admission and three months ago when he was seen in the office.
Mr. Solomon suffered an inferior wall infarction secondary to a ruptured plaque or ulcerated plaque and superimposed thrombus occluding the right coronary artery.
Three months ago, Mr. Solomon suffered angina secondary to ischemia in the LAD which was 80% narrowed.
10. Before we discuss management we need to have a good understanding of patho-physiology of Myocardial infarction. Describe the patho-physiology of atherosclerotic plaque leading to thrombosis.
The evolution of a streak into a plaque occurs in the 2-4th decade of
life with the number of plaques related to risk factors . The key element is the
appearance of extracellular lipid. The lipid first appears in the extracellular matrix
then as a lipid core. The lipid core is primarily acellular with loads of oxidized lipid
and margins surrounded by numerous lipid-laden macrophages. These macrophages express
Tissue Factor which makes the core area the most thrombogenic part of the plaque. The
smooth muscle cells (SMC) produce collagen to encapsulate and limit the lipid core however
activated Macrophages produce enzymes (e.g.…Metalloproteinases) capable of breaking
down the connective tissue matrix. It's a war in there!
An atherosclrotic plaque ulcerates resulting in activation of the platelets and clotting
cascade resulting in an occlusive
thrombus.
The plaques that rupture most often are not the largest, most luminal impinging but most often are <75% diameter stenosis. They have a large core and thin fibrous cap.
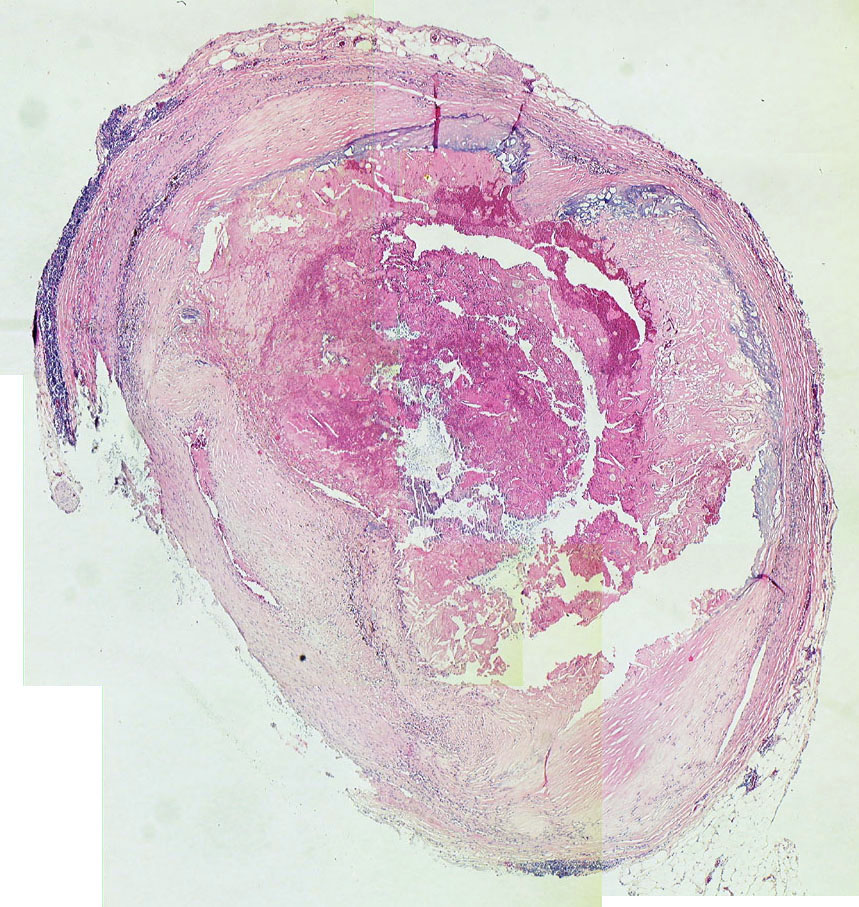
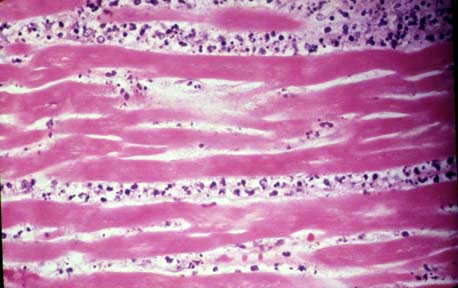
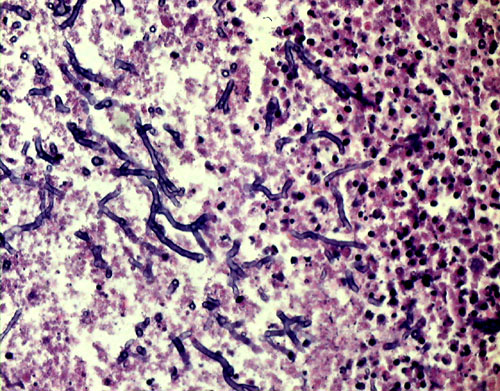
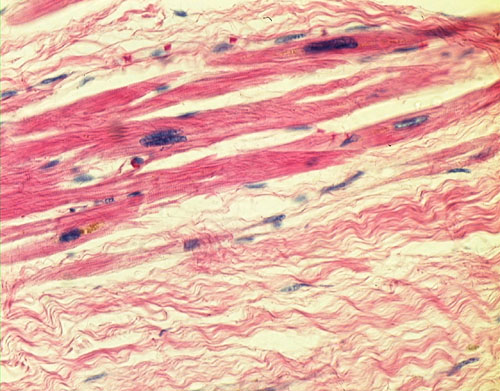
11. Describe the evolution of myocardial changes that occur following acute myocardial infarction.
12. Describe the evolution of clot/thrombus over time.
Thrombosis cab be defined as pathological transition of the state of blood from fluidity to non-fluidity. Initially a stationary thrombus is formed. The stationary clot (thrombus) may progress and eventually break into small pieces which when released into circulation are called emboli. The fibrinolytic system is a network of enzymes that are responsible for the dissolution of a formed clot.
As clots age they are stabilized by factor XIIIa and there is cross-linking of fibrin and the beginning of collagen deposition. These are not lysable at this stage.
13 What are the clinical consequences of acute myocardial infarction?
14. What should be your strategy when you suspect that the patient may have Myocardial infarction in the Emergency room ?
The goals of therapeutic strategy for MI:
15. Mr. Solomon was treated with oxygen by nasal cannula, IV morphine, IV nitroglycerine and IV metropolol upon admission from the emergency room to improve oxygen supply/demand ratio to myocardium. What effect would each treatment have on the oxygen supply/demand ratio of the myocardium?
With a normal arterial pO2, oxygen therapy probably has little effect on the supply/demand ratio of the myocardium.
Morphine has venodilator effects which may cause a reduction in preload, ventricular wall stress and oxygen demand. Also the central effects of morphine to increase vagal tone and reduce the pain-mediated rise in sympathetic tone may also reduce myocardial oxygen demands
Nitroglycerine and metropolol would both decrease oxygen demands in AMI as they do in stable and unstable angina. Although several clinical trials have shown that these agents may reduce the amount of muscles that become necrotic, the reduction in infarct size is minimal compared to what can be achieved by thrombolytic therapy.
Since beta-blockers have been shown to reduce mortality for at least one year following a MI, it is advisable to initiate beta-blocker therapy prior to hospital discharge.
We should limit all activities for a period of time to limit the oxygen demand.
16. What is the role, if any, for aspirin and/or heparin in Mr. Solomon’s treatment?
There is now extensive evidence that thrombosis occurs simultaneously with endogenous (spontaneous) and exogenous thrombolysis. Although aspirin and heparin will not lyse a coronary thrombus, these drugs are essential in preventing re-occlusion. Even during the administration of fibrinolytic agents, episodes of transient reperfusion followed by re-occlusion often precede sustained coronary reperfusion.
17. What are the options to re-establish coronary perfusion? Is it indicated for every patient? How do you select the option?
The object of reperfusion is to prevent myocardial necrosis.
Early reperfusion improves LV function and survival in patients with
Our job is to abort the infarct. Decide (with Cardiology consultation) on the method of reperfusion and "Just do it"
With experienced hands , PTCA may have slight advantage in mortality and complications over Thrombolytic therapy in the short run.
At this point PTCA is equal to not better than thrombolytics.
18 Let us now address Thrombolytic therapy. What is the rationale, if any, for the use of intravenous t-PA in treating Mr. Solomon. How would you gauge the clinical effectiveness of t-PA?
Tissue plasminogen activator (t-PA) converts plasminogen to plasmin which acts to digest the fibrin clot that is occluding one of the major coronary arteries. A decrease in chest pain or reduction in the magnitude of ST-segment elevation in the ECG would suggest that reperfusion had been achieved. Unfortunately, these markers are rather imprecise and coronary angiography is the only definitive method for recognizing successful reperfusion. If a method was available for assessing reperfusion (after 90 minutes of IV thrombolytic therapy) could be transferred to the cardiac catheterization laboratory for rescue angioplasty.
19. How would the latency from the onset of symptoms to the start of t-PA therapy influence the effectiveness of therapy?
In order to salvage reversibly injured cardiac muscle, thrombolytic therapy should be initiated within the first six hours after the onset of symptoms. Beyond six hours cardiac myocytes are irreversibly injured and reperfusion probably does not reduce the ultimate amount of necrosis. There is evidence however, that reperfusion after six hours may help in the healing process with less thinning of the scar and less chance of aneurysm formation. The lack of any benefit after 12 hours may be due in part to the ineffectiveness of thrombolytics in lysing older thrombi. As clots age they are stabilize by factor XIIIa and there is cross-linking of fibrin and the beginning of collagen deposition.
| 0-6 hours | 6-12 hours | >12 hours | |
Clot |
Lysable | Collagen deposition. Not lysable | |
Myocyte |
Still viable | Irreversibly injured/does not reduce extent of necrosis/May facilitate healing process |
Risk of hemorrhagic transformation in the infarcted territory with very little muscle to salvage |
20. List and describe the current thrombolytic agents used to treat patients like Mr. Solomon.
Urokinase
Streptokinase,
t-PA and
Anisoylated plasminogen streptokinase activator complex (APSAC).
T-PA binds to fibrin with greater affinity than does urokinase or streptokinase and activated plasmin on the fibrin surface. In theory, this should lead to a more localized (clot specific) effect and less systemic fibrinolysis. T-PA also has no antigenicity. Although clinical trials have been conflicting, in general, streptokinase and t-PA are thought to produce similar results in terms of vessel patency and overall mortality. Since streptokinase costs only 1/5 to 1/10 as much as t-PA, it is used more often to treat acute myocardial infarction.
21. What are the major risk factors associated with the use of thrombolytic therapy?
Intracrainal hemorrhage and bleeding are the main risk associated with thrombolytics. Lysis of a preformed thrombus at a site of recent stroke or surgery allow for bleeding. Thrombolytic agents should be avoided within 10 days of surgery and 6 weeks of a stroke. Extremely low fibrinogen levels can also result in bleeding as well as impaired platelet function due to lysis of the surface glycoproteins.
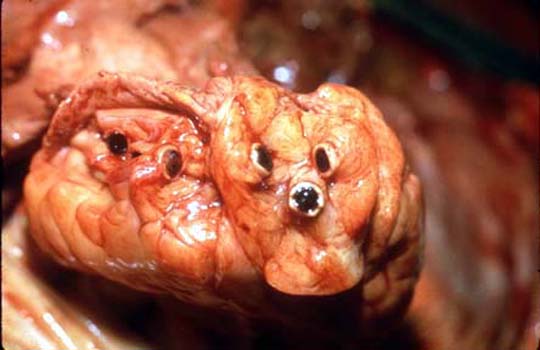
22. If Mr. Solomon presented with a holosytolic murmur heard best at the apex and radiating into the axilla, what would be a likely pathogenesis for this problem? What type of murmur this is, based on the characteristics given in the question. Correlate the physical finding with the pathologic process.
The appearance of mitral insufficiency during the course of an infarct suggests ischemia or necrosis of the papillary muscle. The damaged muscle cannot anchor the mitral valve leaflet to the ventricular wall preventing retrograde flow of blood into the atrium.
23. List complications of myocardial infarction and principles of management of each.
| Ventricular dysfunction | Hypotension/Cardiogenic Shock | IABP, Re-perfusion strategy |
| Ventricular dysfunction | Congestive Heart failure | |
| Irritable focus: | Dysrhythmias | Based on arrhythmia ( Atropine, Lidocaine) |
| Sudden death | ||
| Ischemia/necrosis of bundle of HIS: | Heart block | Pace maker |
| Elevated catecholamine release | Hypertension | |
| Pericarditis | High dose ASA 650 mg q 4-6 hour | |
| Papillary muscle ischenia/necrosis | Mitral regurgitation. Acute valvular dysfunction./Flash pulmonary edema | Emergency Valvular surgery |
| Rupture if interventricular septum | VSD | Requires Surgery |
| Thinning of Myocardium | Ventricular aneurysm | Requires Surgery |
| Ventricular rupture |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}