1. Explain the significance of the following in the protocol that my have a bearing to this patient's chief complaint.
Bloody (Upper GI bleeding): Tarry and sticky with fowl smell
Non-bloody
Therapeutic intake of iron
Pepto-Bismol (bismuth compounds)
Licorice.
Lightheadedness. A sign of low cardiac output secondary to hypovolemia.
Sticky malodorous stools. Not seen with non-bloody black stools.
NSAID's. Can give rise to Gastritis or precipitate bleeding from Ulcers.
Postural hypotension. A drop greater than 10 mm of Hg in erect position.
No telengiectasia. Finding indicating Hereditary hemorrhagic telengiectasia could be the etiology.
No spider nevi. Finding encountered in Cirrhosis suggesting possible esophageal varices as a source of bleeding.
Full Parotid glands. Seen in chronic alcoholics with Cirrhosis.
Type of anemia. Normochromic anemia with acute bleed. Microcytic hypochromic anemia with chronic bleed.
BUN and Creatinine. Absorption of GI blood and decreased renal perfusion,
2. What is the major clinical problem (not the diagnosis)?
Melena (tarry, black stools) is the major clinical problem
3. What is most likely cause for the black stools based on the information you have gathered so far?
Acute GI bleeding
4. What physical findings and lab data support a diagnosis of acute bleeding?
Manifestation of hypovolemia.
Anxiety, lightheadedness, restlessness.
Pale, moist skin.Ā
Orthostasis, tachycardia
Weak peripheral pulses
Absorption of blood
Elevated BUN
Loss of blood
Decreased hemoglobin withĀ normal MCV.
ĀMelena per rectum.
5. What is the likely location of bleeding site in GI tract
Above the ligament of Treitz.
6.What makes the stool blood black?
Hydrochloric acid converts Hemoglobin to
Digestive enzymes act upon the blood and change the color and consistency.
7. What amount of blood loss is required to produce each of the following:
Occult positive stool. 3 cc (hemoccult).
Melena =100-200 cc
Orthostasis=20% loss of circulating volume or about 1000 cc.
8. Now that you have localized the probable area for a bleeding source develop a differential diagnosis for the problem.
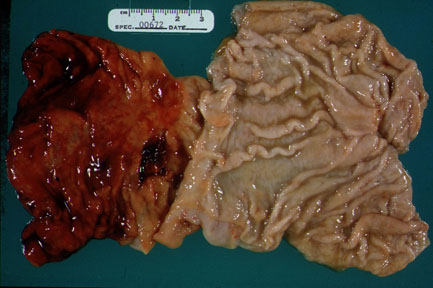
Duodenal ulcer
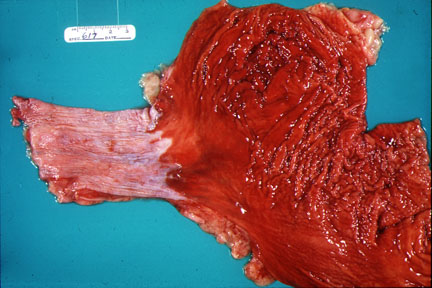
Gastritis (Gastro-duodenal erosions)
Esophagitis (GERD)
Esophageal varices
Mallory-Weiss tear
Arteriovenous malformations
Swallowed blood from hemoptysis or orpharyngeal bleed
9. Discuss the likely diagnosis. Cite data to support your diagnosis. Describe the clinical scenario for other diagnosis that you have listed as possibilities.
Bleeding duodenal ulcer is the most likely diagnosis.Ā
Diagnosis strengthened by epigastric burning with similar episodes in past.Ā
Epigastric tenderness on exam.
The history of alcohol, smoking, NSAIDÆs use, aspirin use.Ā (predisposing factors)
Prior history of "Ulcer"
Lightheadedness, orthostatic vitals.Ā Cool, moist skin, Melena support acute GI bleeding
Elevated BUN.Ā (Pre renal azotemia)
Gastro-duodenal erosions. Abuse of NSAID
Esophagitis (GERD). History of reflux,
Esophageal varices. In a cirrhotic with portal hypertension.
Mallory-Weiss tear. Retching followed by hematamesis.
Arteriovenous malformations. In a patient with stigmata for hereditary hemorrhagic telengiectasia.
Swallowed blood from hemoptysis or oropharyngeal bleed
10. Now that you have the differential, what are the historical information that you will gather in evaluation of acute upper GI bleed?
Stool characteristics
Black
Sticky
Foul smell
Intake of
Iron
Pepto-Bismol (bismuth compounds)
Licorice
Symptoms of hypovolemia
Lightheadedness
Use of NSAID's. Can give rise to Gastritis or precipitate bleeding from Ulcers.
Epigastric distress
GERD symptoms
Retching
Nose bleeds
History of Alcoholism and Cirrhosis
Previous aortic surgery, portal hypertension
11. What physical findings will you be looking for?
Manifestation of hypovolemia.
Anxiety, lightheadedness, restlessness.
Pale, moist skin.Ā
Orthostasis, tachycardia
Weak peripheral pulses
Finding encountered in Cirrhosis suggesting possible esophageal varices as a source of bleeding.
Spider nevi.
Full Parotid glands
Hepatomegaly
Splenomegaly
Finding indicating Hereditary hemorrhagic telengiectasia
Careful exam of Oropharynx for bleeding sites if any
12. Prioritize steps that would likely be taken in the ER to treat this patient.
Brief history/physical exam
Assessing the degree of circulatory compromise by doing orthostatics.Ā
Establish IV access with 2 large bore IVÆs.Ā
Volume replacement.Ā
Type and cross-match for blood.Ā
Nasal oxygen.Ā
EKG.
Laboratory evaluation to include CBC, coags, BUN, creatinine.Ā
Nasogastric tube.Ā
Consult with endoscopist and surgical colleagues.
13. A nasogastric tube was placed by the ER resident. The aspirate reveals a clear return. What does this mean? Does this change or alter your diagnosis?
GI bleeding is often times intermittent and can stop spontaneously.Ā
The clear return suggests a competent pylorus and bleeding could be still occurring in the bulb and going postbulbar.Ā
14. Interpret the possible returns from nasogastric tube
Coffee grounds = slow bleeding or oozing.Ā
Red blood/clots = active ongoing bleed.Ā
Bile stained = no active bleeding above the Treitz ligament. A bile stained NG aspirate would make active bleeding proximalĀ to the third portion of the duodenum most unlikely.Ā
Clear = GI bleeding is often times intermittent and can stop spontaneously.Ā The clear return suggests a competent pylorus and bleeding could be still occurring in the bulb and going postbulbar.Ā
15. What will be the ideal procedure to confirm the location of bleeding site and why?
Once the patient has stabilized (No orthostasis, slowed pulse) an upper GI endoscopy (EGD) would be the procedure of choice.Ā
EGD is diagnostic and can be therapeutic if active bleeding or visible vessels are seen.Ā
Injection therapy with epinephrine or a variety of electro coagulation techniques can be used to stop bleeding.
EGD in this cases would rule out varices (a cause of severe UGI hemorrhages) which was an initial consideration.Ā
Also the EGD could permit a biopsy to evaluate for Helicobacter pylori, a causative agent in most peptic diseases.Ā A biopsy would be taken from an area of the antrum, not from or in close vicinity to bleeding lesions.Ā
16. 70/plus% of UGI bleeds will cease spontaneously. What is the advantage of doing EGD in every case?
The EGD can provide useful information (diagnosis) as well as being therapeutic in needed instances.
Tissue can be obtained.
The endoscopic findings can help assess the risk for recurrent hemorrhage (rebleeding increases mortality)
17. List factors that increase the mortality and morbidity from UGI bleeding.
Rebleeding after initial presentation.Ā
Severity index of bleeding (transfusion requirement, BRB/NGT, hypotension).Ā
Variceal bleedĀ
Age>60.Ā
Multisystem disease (co-morbidity).Ā
Endoscopic stigmata of recent bleeding (Active bleeding, visible vessels, fresh clot).Ā
Onset of bleeding in hospitalized patient.Ā
Need for emergency surgery for bleeding.
18. What are the endoscopic findings suggesting increased risk for rebleeding?
Redspot/Ulcer base 10%
Clot 20%
Visible vessel 50%
Clean base Negligible
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}