Emphysema
Definition
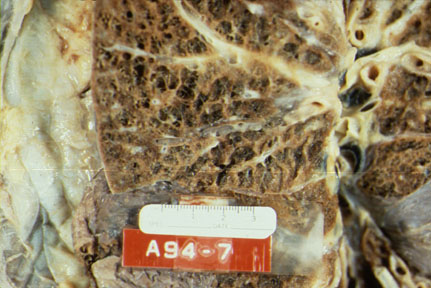
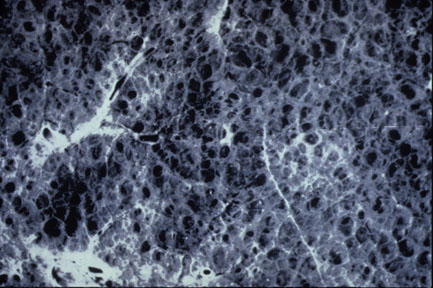
Emphysema is a pathologic condition of the lung defined as abnormal Emphysema airspaces
Classification.
Although the definition of emphysema describes the basic pathology, this disease can be
further divided into four subgroups based on the part of the respiratory acinus (lobule)
which is damaged and the location of these damaged lobules within the lung. (Refer to 15-8 and 15-9 in your
textbook).
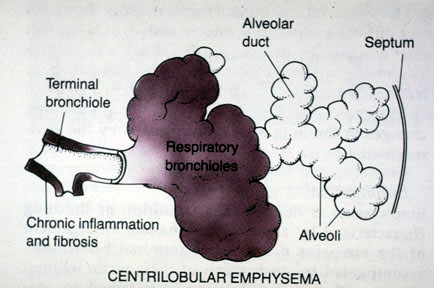
- Centriacinar
Emphysema:
- Involves primarily the respiratory bronchiole (proximal
and central part of the acinus is expanded)
- The distal acinus
or alveoli are unchanged.
- Occurs more commonly in the upper lobes.
- Most common type.
- Seen in cigarette smokers
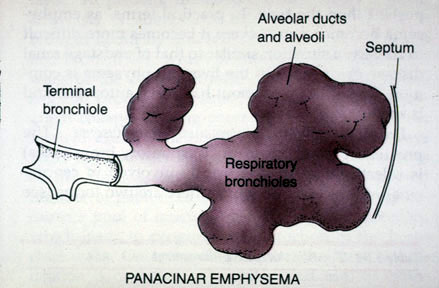
- Panacinar
Emphysema:
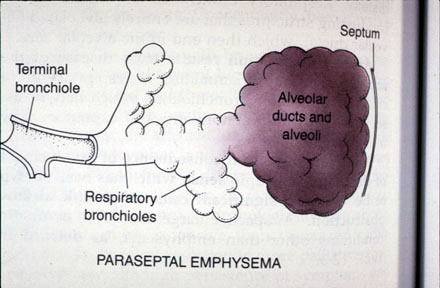
- Distal acinar (Paraseptal emphysema):
- The distal respiratory acinus, including alveolar duct and alveoli, is expanded.
- Occurs primarily adjacent to the pleura and connective tissue septa, especially
in the upper lobes.
- Extensive involvement of the lung is rare.
- Some cases of spontaneous pneumothorax may be due to this type of emphysema
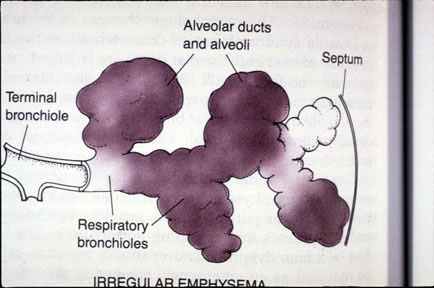
- Irregular:(
Paracicatritial emphysema)
- Irregular emphysema is associated with scarring
- No particular relationship to the acinus .
- Bullous emphysema, by definition, is composed of lesions > 1
cm in diameter, and can be associated with any type of emphysema
- A bleb is a localized pocket of interstitial emphysema,
typically subpleural, with no destruction of lung tissue
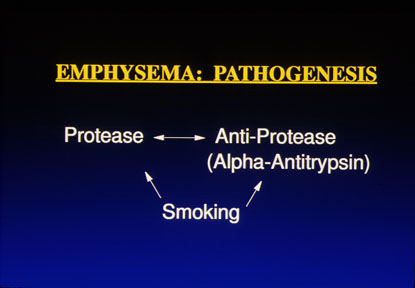
Pathogenesis
- Emphysema is associated with heavy cigarette smoking. But how
does smoke damage the respiratory acinus?
- Protease -
antiprotease theory: The walls of acinus are destroyed when there is an imbalance
between proteases and anti-proteases in the lung. Protease is an enzyme like elastase,
which can digest connective tissue elements. Proteases are found throughout the body,
especially in neutrophils and macrophages. To counterbalance the destructive effects of
proteases, nature provides inhibitors such as alpha-antitrypsin.
- Smoking increases the level of lung proteases while impairing the action of
anti-proteases. Patients with panacinar emphysema may lack alpha-antitrypsin.
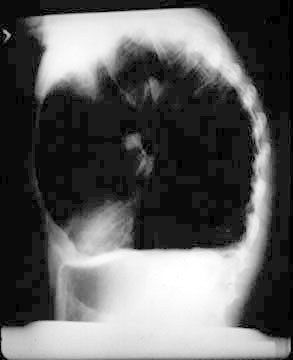
Pathophysiology
Progressive dyspnea,
over inflated lungs, barrel chest, hyperresonance,
and distant breath sounds.
Chronic bronchitis
Definition
- A patient has chronic bronchitis when he or she has a
- persistent, productive cough
- for at least 3 months
- in at least 2 consecutive years.
- Although chronic bronchitis is defined officially in clinical terms, this
condition is a chronic inflammation of the trachea, bronchi and bronchioles which is
characterized by hypersecretion of mucous and thickening
of the walls of respiratory tree.
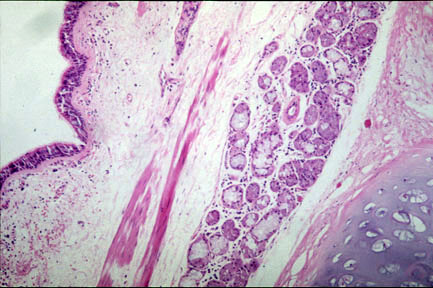
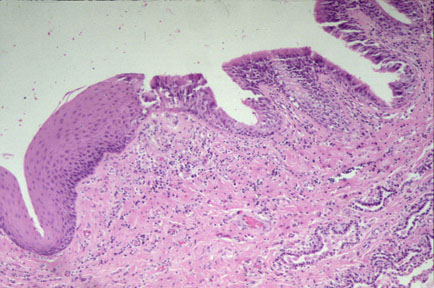
Pathology
How are the tubes of the respiratory tree narrowed? The histologic features are
- Chronic inflammation of bronchi (usually lymphocytic)
- Marked increase in the size of the mucus secreting glands of the
submucosa in the trachea and large bronchi with excessive mucus
secretions in the lumina of the respiratory tree. The Reid Index is a ratio of the
thickness of the gland layer to the thickness of the submucosa. The Reid index measures
the gland to wall ratio
(normally glands are 1/3
of wall thickness as measured from epithelial basement membrane to cartilage). The
ratio is increased in chronic bronchitis.
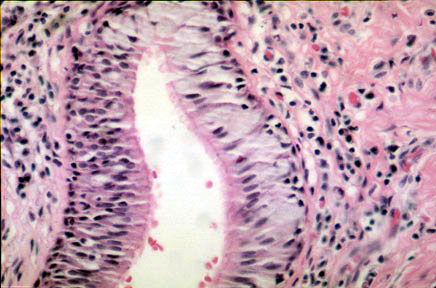
- Hyperplasia of goblet
cells in small bronchi and bronchioles.
- Squamous metaplasia and
dysplasia of bronchial epithelium.
Pathogenesis
- Inhaled irritants such as smoking.
- Infections.
Pathophysiology
Persistent, productive cough; dyspnea; expiratory wheezing. Chronic bronchitis:
Clinical picture
Corpulmonale
Central cyanosis
Cyanosis
Mechanics of breathing
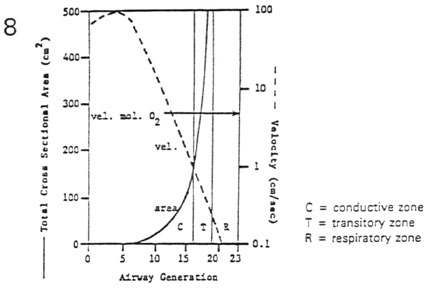
Air Flow Profiles in the Airways
- Cross-Sectional Area
of the Airways
- total cross-sectional area increases exponentially with generation (solid line)
- forward air flow velocity decreases exponentially with generation (dashed line)
- Three Types of Air-Flow Profiles
- continuity equation
- flow (mL/sec) = vel (cm/sec) * cross-sect area (cm2) * (mL/cm3)
- Reynold's Number (NR) = density * mean velocity * diameter / viscosity
- turbulent flow for NR > 3000 (gen. 0-6)
- laminar flow for NR <2000 (gen. 7-17)
- diffusive flow with cardiogenic mixing for NR
= 0 (gen. 18-23)
Four Factors Affecting Air-Flow Resistance
- Airway Caliber
- laminar flow (
 ) =
) =  pressure (P) /
resistance (R)
pressure (P) /
resistance (R)
- slope of line = 1/R = conductance
- resistance (R) to laminar flow
 1/radius4
1/radius4
 airway caliber (secretions,
bronchoconstriction): <
airway caliber (secretions,
bronchoconstriction): < R and < P
R and < P
- Air-Flow Profile
- laminar flow (<) increases linearly with < driving pressure
- non-laminar flow (<) increases curvilinearly with < driving pressure
- Rnon-laminar flow is effectively greater than Rlaminar flow
due to turbulence
- for any given < P, <non-laminar <<laminar
- or any given <, <Pnon-laminar > < Plaminar
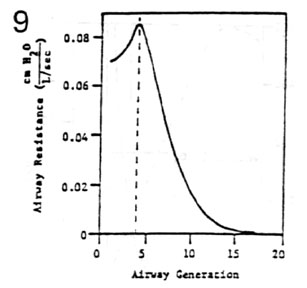
- Airway Generation
- in general, regional airway resistance decreases as a function of airway
generation
- in specific, the highest regional resistance is at generation 4
- medium sized bronchi of short length and frequent branchings highly non-laminar
air flow with extreme turbulence
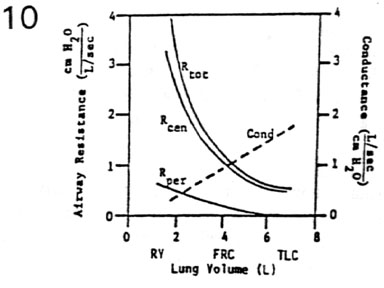
- Lung Volume
- total airway resistance = summation of serial regional resistances
- Rtotal decreases hyperbolically with increases in lung volume
- conductancetotal increases linearly with increases in lung volume
(dashed line)
- increases in lung volume cause increases in radius due to tethering of the
airways
- Rtotal can be partitioned into two components
- Rperipheral (gen. 7 - gen. 23): low resistance (laminar &
diffusive zones)
- Rcentral (nose - gen. 6): high resistance (turbulent flow zone)
- Rcentral >>> Rperipheral (50% of resistance in
nasal passages alone)
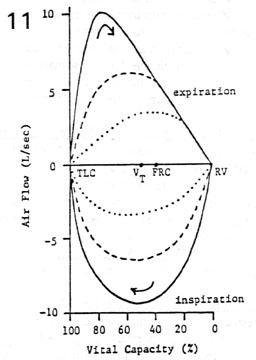
Dynamic Compression of the Airways
- Flow-Volume Loops
- air flow (L/sec) is plotted against lung volume (% Vital Capacity)
- inspiratory and expiratory air flows form a closed loop (clockwise rotation)
- for any lung volume, max inspiratory air flow is effort dependent
- for high lung volumes, max expiratory air flow is effort dependent
- for low lung volumes, max expiratory air flow is effort independent
- Dynamic Compression of the Airways
- the expiratory portion of the maximal flow-volume loop has a scooped- out
appearance
- during active, forced expiration Ppleural can actually exceed Pairway
- this transmural pressure gradient favors airway compression (Starling resistor
effect)
- greater effort ( Ppleural)
results in greater compression ( radius) with no
change in air flow
- compression starts at the equal-pressure point (EPP) in the cartilage-free
airways within the lung
- in disease the weakened airways can actually collapse causing air-trapping behind
the blockade
- lip pursing moves the EPP to the mouth, a psychological relief to the patient
Work of Breathing
- Components of Work
- elastic work - work to overcome:
- lung elastic recoil
- thoracic cage displacement
- abdominal organ displacement
- frictional work - work to overcome:
- air-flow resistance (major)
- viscous resistance (lobe friction, minor)
- inertial work - work to overcome:
- acceleration and deceleration of air (negligible due to low mass of air)
- acceleration and deceleration of chest wall and lungs (negligible due to
overdamping)
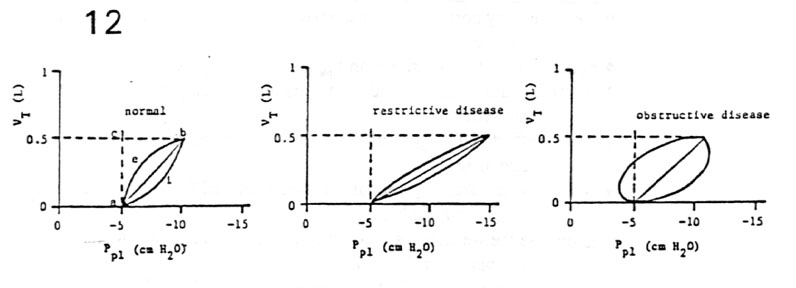
- Graphical
Representation of the Major Components of Work
- work = force * distance
 pressure
* volume / 2
pressure
* volume / 2
- elastic work area a-b-c-a
- inspiratory flow-resistive work
 area a-i-b-a
area a-i-b-a
- expiratory flow-resistive work area
a-b-e-a
- negative work area a-e-b-c-a (tone
on inspiratory muscles during expiratory air flow)
- total work Welastic + Winspiratory
flow-resistive + Wnegative
- passive recoil of lungs overcomes the work of expiratory flow-resistance
- Work of Breathing in Disease
- restrictive or low compliance diseases (e.g. fibrosis)
- Welastic + normal Wflow-resistive
+ Wnegative = Wtotal
- obstructive or high air flow resistance diseases (e.g. asthma)
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}