Definition
- Pulmonary abscess is a localized area of liquefactive necrosis of the
lung.
- This would then include necrotizing gram negative and gram positive pneumonias
eg. Klebsiella, Staph, Pseudomonas etc.
- However, by convention we reserve the term lung abscess for necrotizing anaerobic
pneumonia.
Prerequisites and Predisposing Conditions
- Aspiration of a Large Bacterial Inoculum:
The aspiration of oropharyngeal contents with a bacterial bolus inoculum is the
prerequisite for development of lung abscess.
- Loss of Cough Reflex:
If the cough reflex is intact, significant aspiration is not possible unless it is
overwhelming. Altered sensorium is the most common state when cough reflex is suppressed,
thus CVA, drug overdose, alcoholism, post-op state or coma from any cause is the most
common predisposing factor for lung abscess.
- Trouble with Deglutition:
This occurs with neurological disorders and esophageal diseases. Aspiration to lungs is
frequent in this situation even if the cough reflex is intact. In many of the Esophageal
diseases the mode of presentation is Lung abscess.
- Post Obstructive Pneumonia:
Lung abscess can occur as a complication of post obstructive pneumonia as seen in some
patients with lung cancer or foreign body aspiration.
Common Segments
- The superior segments of RLL, LLL and axillary subsegments of anterior
and posterior segments of RUL are common sites for aspiration and will account
for 85% of all Lung abscesses.
- Gravitational forces determine the site of aspiration. Position
of the patient at the time of aspiration determines the segment the aspiration is most
likely to occur.
- Basal segments of RLL used to be the most common site for aspiration during 1940
to 1960. During this period ENT surgery and Dental work was done in sitting position with
Ether as the anaesthetic. The Right main bronchus is in straight line with Trachea while
left main takes of at an angle. In this position gravity facilitates lodging of the
aspirate to basal segments of RLL.
- In supine position and with the patient on back superior segment of RLL is the most
dependent segment.
- In right lateral decubitus position the axillary subsegments of anterior and
posterior segments of RUL is the dependant site for aspiration. Abscess is located in the
middle of lateral CXR corresponding to RUL bronchus take off.
- When the patient is on abdomen, aspiration does not occur, thus it is extremely
unlikely for any anterior segments, middle lobe and lingula to be the site for aspiration
lung abscess. When lung abscess is encountered in these sites on should suspect partial
airway obstruction or trouble with deglutition as the
predisposing factor for lung abscess.
Clinical Picture
- Most of the patients present with subacute onset of illness and
do not seek medical attention for three to four weeks since the onset of illness.
- Patients complain of cough, low grade fever, anorexia and weight loss of few
weeks duration .
- Patients often have cough with large amounts of foul smelling sputum.
- Lack of foul smell does not exclude lung abscess, as 50% of anaerobic infections
do not produce a foul smell.
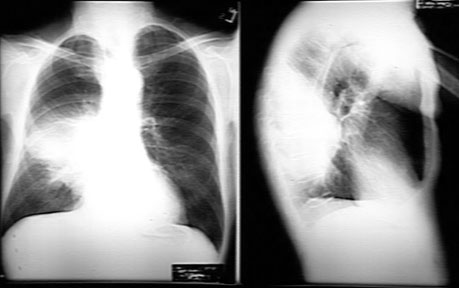
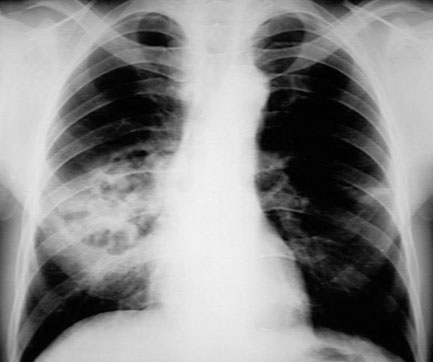
Radiogical features:
- The superior segment
of RLL , LLL and axillary sub-segments of anterior and posterior segments of RUL usually
account for 85% of all aspiration lung abscesses. The lesions will correspond to these
sites in CXR.
- In the early stages one sees consolidation.
- The inflammatory mass eventually necroses and the necrotic material is
expectorated through bronchus.
- The cavity that results has thick wall with irregular lumen.
You may note stalactites and stalagmites in the lumen.
- Air fluid level is
the hall mark of Lung abscess.
- The appearance of the cavity is similar to necrotizing squamous
cell cancer of lung and has to be differentiated from it.
Bacteriology
Common pathogens are
- Gram positive anaerobes such as peptococci and peptostreptococci,
the micro-aerophilic streptococci which are part of normal oropharyngeal
flora
- Gram negative anaerobes such as the prevotella (P.
Melaninogenicus), Fusobacteria (necrophorum and nucleatum).
Definition
Pulmonary abscess is a localized area of liquefactive necrosis of the
lung.
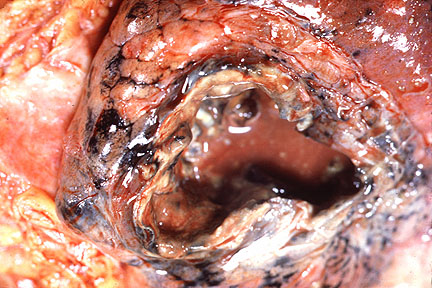
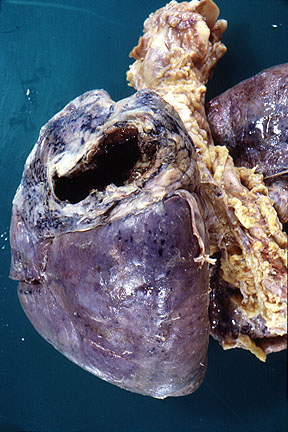
Pathology
The abscess is characterized by
destruction of lung tissue forming a cavity. The cavity is filled with pus (necrotic
debris/liquid) or pus and gas (air). The content of the abscess is extremely foul
smelling. The abscess may be large or small, single or multiple.
Method of Obtaining Specimen
The options are as follows:
- Sputum Gram Stain:
May occasionally be helpful if there is a large number of white blood cells and bacteria
consistent with oropharyngeal flora.
- Bronchoscopy:
- Triple lumen catheter: Routine aspirates during bronchoscopy is useless for
anaerobic cultures. The bronchoscope passes through oropharynx and will be contaminated by
the oropharyngeal flora. You need to use triple lumen catheter to avoid contamination and
obtain material selectively from the involved segment.
- Bronchial lavage: The second option is to obtain a bronchial lavage from the
involved segment and perform quantitative bacterial cultures.
- Fine Needle Aspiration:
In the pre-antibiotic era needle aspirations of lung abscess were fraught with fear of
development of bronchopleural fistula and empyema. With the current option of FNAB under
CT guidance, it is being done with increasing frequency and safety. Uncontaminated
aspirate can be obtained by this method for cultures. This procedure is often the method
of choice for obtaining the specimen in children as other options are not easily feasible
in this population.
- No Need for Cultures:
When the patient has foul smelling sputum the anaerobic infection is obvious and there may
not be a need for confirmation, as many of these procedures are expensive and attendant
with some risks. Most of the lung abscess respond to empiric therapy. The primary purpose for culture is to obtain antibiotic sensitivity and can be
reserved to cases not responding to empiric therapy.
Antibiotic of Choice
- Traditionally, penicillin alone was used and produced
satisfactory results. Of late, there has been increasing incidence of penicillin
resistance in oropharyngeal anaerobes. Hence, penicillin alone is no longer recommended.
- Metronidazole alone has failed despite its superb anaerobic spectrum due to lack
of activity against microaerophilic streptococci which are significant pathogens in lung
abscesses. Penicillin added to metronidazole is an acceptable
alternative.
- Clindamycin is the most popular antimicrobial for treatment of
lung abscesses and has produced excellent results. The intracellular uptake of clindamycin
and its stability in abscess which have low pH and poor vascularity may offer an
advantage.
- Other beta lactams such as ampicillin and sulbactam, ticarcillin
or amoxicillin with clavulanate, piperacillin with tazobactam, cefoxitin and cefotetan
also have excellent activity against anaerobes and offer expensive alternatives. Imipenem
also has excellent activity against anaerobes.
- Presently, available quinolonoses such as ciprofloxacin, norfloxacin, oflaxacin,
etc. have very poor activity against anaerobes and streptococci.
Prolonged treatment over several weeks is typically required.
Methods of Drainage
Role of Bronchoscopy
- Diagnosis:
In the past bronchoscopy was done routinely in all patients with lung abscess with the
intent of detecting foreign body or cancer. In most the bronchoscopy was non-contributory.
Lung abscess is due to aspiration of bacterial bolus and not due aspiration of large
foreign body. Cancer and foreign body aspiration account only for a small number of cases.
Nowadays bronchoscopy is reserved only when the lung abscess is located in atypical
segments or is refractory to therapy.
- Specimen Collection:
As discussed under specimen collection methods, bronchoscopy is one method by which we can
collect specimen for cultures and sensitivity studies.
- Drainage of Pus:
Bronchoscopy is also useful to drain lung abscess
trans-bronchially in selected cases.
Role of Surgery
- In the pre-antibiotic era surgery was the only method of therapy for lung
abscess.
- In the modern era there is very limited role for surgery in patients with lung
abscess.
- Most of the lung abscesses are curable with antibiotics and postural drainage.
- Massive hemoptysis is often the most common indication for surgery in the modern
days.
- In patients with partial airway obstruction, lung abscess may increase in size
even with antibiotics and one may have to resort to drainage procedure or surgical
resection.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}