
|
|
|
|
inflammation.
lymphocytosis.
veryfocal.
material.
|
|
|
|
lymphocytosis.
lesion.
portal-portal.
in hepatocytes.
|
Historical Data After the agents for viral hepatitis A and B were identified in the 60s and 70s it was evident that there was a group of hepatitides caused by some other virus which would infect by blood and would be ultrafiltrable. This elusive virus was called " non-A, non-B". It took 20 years to demonstrate its existence by nucleic acid analysis and still in 1996 we cannot see it with electron microscopy The reason is that its concentration in the blood is very low, probably 1-10 virions per ml.
|
|
Discovery It took 5-6 years of work to extract it from infected patients by a group of investigators in California (USA),(Choo et al, Science 244:359-361,1989). The serum was concentrated into a pellet. RNA was extracted from this pellet and its complimentary DNA (cDNA) placed into the genome of E. Coli. Numerous clones of this organism were tested by Enzymatic Immuno Assay technique (EIA) against the serum of patients convalescent of non-A non-B hepatitis until one clone was found producing a small protein that reacted with IgG from the serum of these patients.. The reacting antigen was called c-100 and the infective agent, Hepatitis C Virus (HCV).
|
|
Virology The virus contains a single-stranded genome of RNA with approximately 10,000 nucleotides, a capsid, a matrix and an envelope. It encodes a single polyprotein precursor which is fragmented in 3 structural (C, E1, E2) and in 4-6 non structural proteins (NS1, NS2, NS3, NS4, NS5) forming the following antigens: c100, c22, c33, c300, 5-1-1 Other components are proteases, RNA polymerase and transcriptases, not reverse transcriptase. We don't know the structure of the HCV because the virus has not been seen yet with the electron microscope due to the very scarce concentration of viral particles in the blood and tissues. Probably only 1-10 virions per ml are present in the blood. HCV appears to be similar to flaviviruses which produce only acute illnesses especially in animals, the prototype being yellow fever virus. HCV does not integrate into host DNA like Hepatitis B virus. HCV has very high mutation rate producing many similar species. This variation accounts for resistance to antibodies.
|
|
Transmission The transmission is by contaminated blood and blood products. Before screening was available, 90% of post-transfusion hepatitis was due to Hepatitis C, now only 5%. Practically all hemophiliacs were infected. It is rarely or not at all sexually transmitted especially among monogamous partners. Hepatitis C carriers should not donate blood , organs or semen. Maternal-infant transmission is low.
|
|
Clinical Course Incubation period is 2-26 (mean. 7.8 ) weeks, Most infected patients, 80-85%, are asymptomatic. Circa 25% of post blood transfusion patients are symptomatic and develop jaundice and ALT to high levels. 40 % of all infected patients develop a chronic course. Almost all chronic hepatitis C infections do not improve spontaneously. The infection persists mostly in a mild chronic form and only a minority of cases develop cirrhosis and/or hepatocellular carcinoma. The complications are greatly influenced by alcohol. In Mild chronic cases the disease does not deteriorate in about 2/3 of the cases. It progresses to moderate or severe chronic active forms in about 1/3 and ends in cirrhosis in fewer than 10 %. In moderate cases, 50% will progress to more severe chronic forms. In all Severe cases usually the disease progress to cirrhosis. Progressive cases should be identified and should receive interferon treatment. Histology is a valuable predictor of progression. These evolutionary changes develop slowly, in an average of 15 years. In summary, viral hepatitis C has a long natural history with mostly benign course, therefore, the frequency of death from all causes in long-standing hepatitis C patients and in controls is identical.
|
|
Complications 1--Cirrhosis may take 10-20 years or more to appear and will have a long indolent course. In exceptional cases (hypogammaglobulinemia, HIV) cirrhosis may have a rapid 5 year course. 2--Hepatocellular carcinoma develops in the presence or absence of cirrhosis. (De Mitri,J hepathology 21(suppl 1):S17, 1994).It may take 30-60 years to appear. HCV RNA can be demonstrated in the tumor as well as in surrounding liver tissue although HCV RNA cannot be integrated in the hepatocytic DNA. 3--Essential cryoglobulinemia-which produce purpura, arthralgia and weakness. Relationship between HCV and cryoglobulin in not clear. 4--Porphyria cutanea tarda due to decrease of Uroporphyrinogen Decarboxylase consists of cutaneous vesicles in exposed areas. 5--Lichen planus. It can be exacerbated by alpha-interferon treatment. 6--Mooren's corneal ulcers. They improve with alpha-interferon.
|
|
Infection in special subjects 1-Children The course is similar to that in adults. There is no growth retardation. Children don't die of hepatitis C because in this disease cirrhosis takes 10-20 years to develop and cause death. Treatment with alpha-interferon has produced same results as in adults. 2-Pregnancy No problems in the development of the fetus. Perinatal transmission is less than 5%. Perinatal Gamma Globulin administration has no benefit. Prenatal screening of pregnant women for hepatitis C is not recommended. HCV is not detected in milk. 3-Renal diseases The incidence of patients on dialysis affected by membranous glomerulopathy and positive for HCV is high but they may acquire HCV infection through blood transfusions, infected organs and instrumentation. HCV does not appear to be directly nephrotropic besides being hepatotropic. Infected patients on dialysis should, therefore, be isolated from non-infected patients both by dialysis machine and by area. HCV infection does not influence the outcome of renal transplants.
|
|
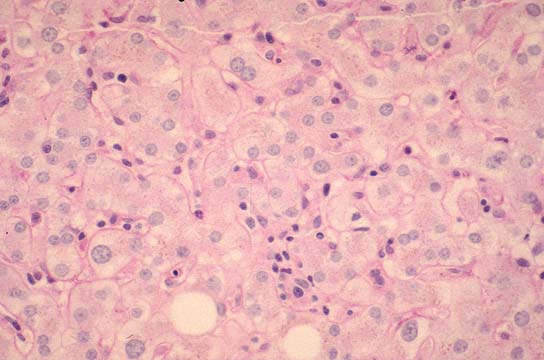
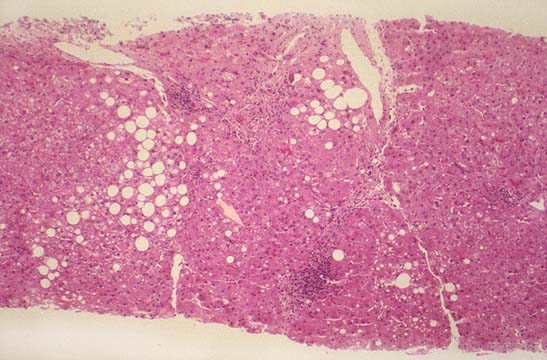
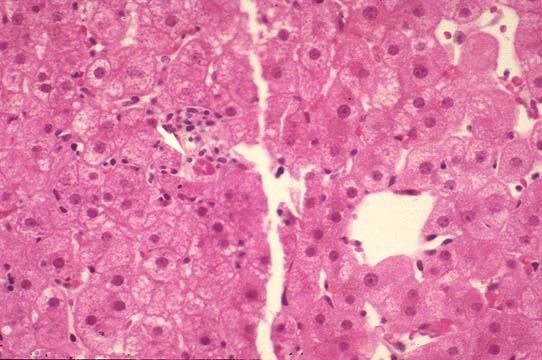
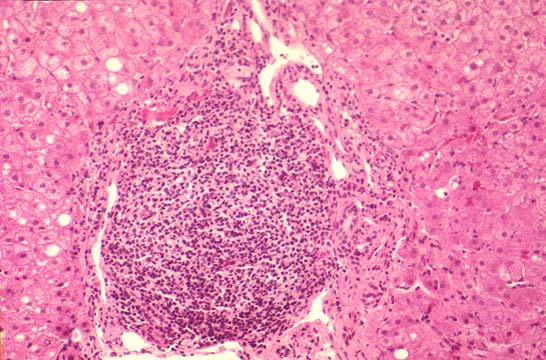
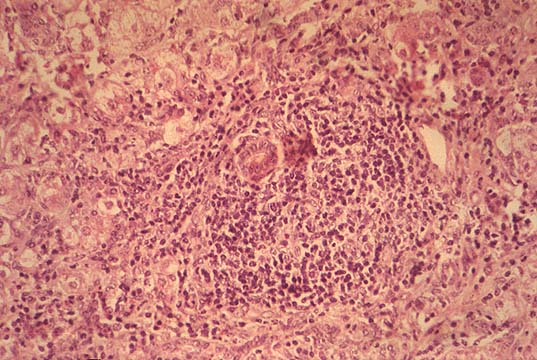
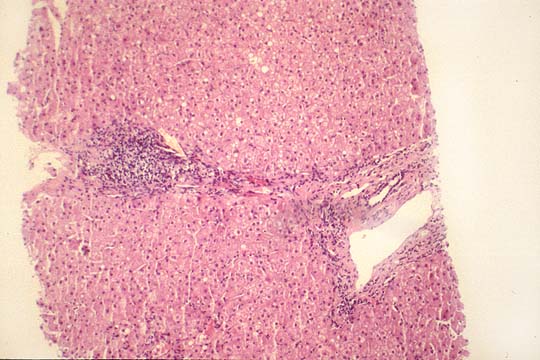
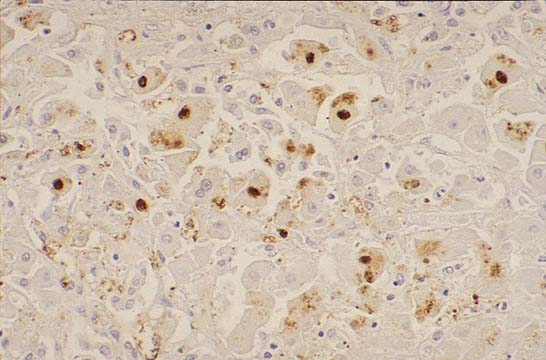
Pathology Viral hepatitis C infection induces the general changes of hepatitis, namely, necroinflammation and fibrosis. These two parameters are morphologically estimated according to the scoring system presented in the discussion of viral hepatitis B. (see contents, li-5-3).As in hepatitis B, the damage of hepatocytes is considered to be immunomediated, (Acadia, Intervirology 37(2):126-132,1994), Although direct viral cytopathogenicity is also probable. A few quantitative differences of pathological changes appear to be associated more with hepatitis C: 1--a mild but constant necroinflammation in the parenchyma.(Gerber, Ver. Deu..Ges. Path. 79:162- 70,1995).( lobular hepatitis). 2--more common lymphocytosis in sinusoids. 3--a strong lymphocytic infiltration of portal fields. 4--epithelial damage of portal bile ducts. 5--macro and microvesicular steatosis. 6--Mallory body-like material. (Lefkowitch, Gastroenterology 104:595-603,1993). 7--hemosiderin granules in endothelium of portal and septal venules. (Kaji, Human Path. 26(10): 1080-5,1995). 8--perivenular fibrosis similar to alcohol.(Uchimura, Liver 15(6):300-6, 1995) HCV antigens can be detected in the cytoplasm of infected hepatocytes with antibodies especially in frozen tissue with immunohistochemistry. HCV RNA can be detected in fixed liver tissue by in situ hybridization. This test is more sensitive than immunohistochemistry.
|
|
|
|
| ||||
| Fig. 115 - Lobular inflammation. |
Fig. 116 - Sinusoidal lymphocytosis. |
Fig. 117 - Steatosis veryfocal. |
Fig. 118 - Mallory-like material. |
||||
| | |||||||
|
|
|
| ||||
| Fig. 119 - Portal lymphocytosis. |
Fig. 120 - Bile duct lesion. |
Fig. 121 - Fibrosis portal-portal. |
Fig. 122 - HCVAg in hepatocytes. |
|
Laboratory Diagnosis 1-Serological tests for HCV specific antibodies. a)(EIA). Enzyme Immuno Assay. HCV has multiple antigen proteins. Serological testing for these proteins forms the basis for demonstrating the infection. The first test consisted of enzyme immunoassaying for one protein, c100-3 (EIA-1).Assaying for multiple antigen by same enzymatic method improved sensitivity to 94-100% and specificity to 97%. False negative results were seen in: -- patients tested before seroconversion ( before developing antibodies to HCV antigens) -- immunosuppressed patients (HIV, organ transplants). --viral heterogeneity (viral mutant different than USA predominant virus (type 1a). False positive results were seen in: --hypergammaglobulinemia. --connective tissue disorders. b) (RIBA). Recombinant Immuno Blot Assay. It is performed on a cellulose strip. Four HCV antigens are blotted and reacted with patient's sera. Reactivity in at least 2 bands (RIBA-2) indicate positive results which are obtained in 85% of patient infected with HCV. 2-Direct demonstration of HCV RNA by PCR. The viral RNA from whole blood ,serum, plasma, fixed tissues, is converted to complimentary DNA (cDNA) by reverse transcriptase and then amplified by PCR. This is a highly sensitive and highly specific confirmatory test. There are ,however false negative but not false positive results. The test is especially useful to monitor the effectiveness of the interferon treatment. For this purpose: 3-Quantification of HCF RNA has been developed. The test results could separate responders from non-responders to treatment. 4-Determination of HCV genotypes will also help in the determination of aggressivnes, possible outcome and management of the infection. There are conflicting reports as to which genotype is more aggressive and which is more benign. It seems that type 1b is more aggressive responding less to interferon therapy and requiring more liver transplants, type 2 seems to be more benign and responds better to interferon treatment. This test with serology and morphology will have a determining place in the management of hepatitis C.
|
|
Differential Diagnosis There are two conditions that can be confused with hepatitis C: 1-- Autoimmune chronic active hepatitis. 2-- Alcoholic liver disease. Instances have been reported of patients who were treated with alpha-interferon for hepatitis C without any result and responded dramatically to cortisone therapy indicating presence of an autoimmune hepatitis. According to a most recent report from Germany"distinction between autoimmune liver disease and viral hepatitis C could be made reliably on clinical and laboratory grounds and----a link between hepatitis A, B, or C virus infection and autoimmune liver diseases is high unlikely".(Lohse et al, Zeitschrift fur Gastr. 33(9):527-33,1995).In case of doubt it is better to try first treatment with cortisone than with alpha-interferon. Alcohol seem to aggravate hepatitis C, actually "patients with hepatitis C who develop cirrhosis under age 50 are those who consume alcohol daily". (Bader, Viral hepatitis, page 141, H&H publishers, 1994).Thus, patients with alcoholic liver disease should be tested for hepatitis C especially if rapid deterioration of the "alcoholic" cirrhosis is observed.
|
|
Medical Treatment Alpha-2- interferon The existing treatment is , so far (1996) alpha-2b interferon, which is of long duration, with serious side effects and expensive. It produces temporary results in about 40% and permanent results in only 20% of the patients. The best responders are those cases without cirrhosis, without severe inflammation , with low serum ferritin, low serum GGT(Gamma-Glutamyl Transpeptidase), low body weight, low viremia HCV. In a series of patients who remained viremic after a sustained biochemical response to interferon therapy 53% of the cases positive for HCV RNA relapsed in a 4 year time. Test for HCV RNA 1 year after a sustained biochemical response to interferon therapy should be done to determine whether the response is complete and permanent. (Chemello Ann. Int. Med. 124(12):1058-60,1996). Positivity for HCV RNA was encountered in patients who were older, had received smaller doses of interferon and were infected more frequently with HCV genotype 2. |
|
Surgical Treatment Liver transplantation It appears that reinfection of transplanted liver in pre-transplant recipients positive for HCV RNA is universal. Its course also appears to be not as indolent as it was thought. In the following report (Greenson, Am. J. Surg. Path.20(6):731-8,1996): --all post transplant biopsies were positive for HCF RNA. --positivity reappeared between 12 days and 4 years. --78 % of patients developed recurrent chronic hepatitis. --chronic hepatitis of acute lobular type appeared in an average of 135 days. --chronic hepatitis with portal lymphoid aggregates appeared in an average of 1 year. --53 % of lobular hepatitis progressed to chronic hepatitis. --30% developed progressive fibrosis. --10% cirrhosis. --0.05% died of liver failure. |
|
Prevention At present time Gamma Globulin (ISG) is not recommended for prevention of post- exposure hepatitis C. Neutralizing antibodies against this infection may not exist. Pre- exposure prophylaxis with Gamma Globulin seems to be effective as proven by the "vaccination"program conducted on over 100,000 USA soldiers in Korea. (Conrad, J. Infect . Dis.;156:56-63,1987). |