1. Define all unknown terms:
Angina:
Clinical Syndrome
Myoacrdial ischemia
Precordial discomfort
Precipitated by exertion
Relieved by rest or sublingual Nitroglycerin
Radiation: Pain secondary to Myocardial ischenia or injury can radiate along medial aspect of left arm, to jaw , shoulders and epigastrium. Pain of Ureteral stones can radiate down to genitals. Pain of dissecting aneurysm radiates to back.
Apical Heart rate: Pulse rate and apical rate should be the same when the heart is regular. If it is irregular the heart rate can be higher than pulse rate.
S4: Fourth heart sound. Heard when the compliance of the myocardium is stiff. (Hypertension, Aortic stenosis)
R2ICS: Second right intercostal space.
Apex: The lower and outermost detectable cardiac impulse.
Indirect Inguinal Hernia: The hernial sac is a patent processes vaginalis and the neck of the sac is situated at the deep inguinal ring, lateral to the inferior epigastric artery.
Direct Inguinal Hernia: protrudes directly through the posterior wall of the inguinal canal, medial to the inferior epigastric artery.
2. Cite the primary clinical problem (not the diagnosis)
Chest discomfort or pain
3 .Develop a general differential diagnosis of this clinical
problem using categories of disease. Cite examples from each:
The objective is intended to help you understand that a given
clinical problem or complaint may have many different causes. You should be aware that chest pain may arise
from different organs or anatomical locations.
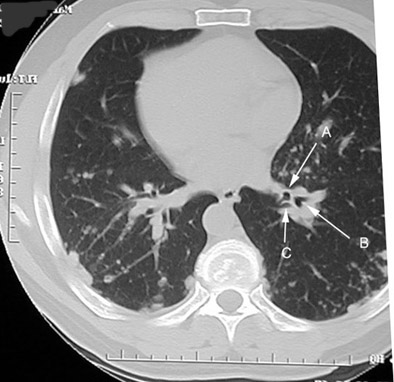
CT chest showing structures in Thorax
Cardiovascular: Angina
Acute myocardial infraction
Pericarditis
Aortic dissectionGastrointestinal: Reflux esophagitis
Esophageal spasm
Esophageal rupturePulmonary: Pneumothroax
Pleuritis/pneumonia
Pulmonary embolus/infarctionMusculoskeletal: Traumatic injury
Costochondritis
Herpes zosterSomatization: Anxiety
4. In general, what factors (data) would you take into
consideration when determining a differential diagnosis of specific diagnosis:
History
Nature and characteristics of complaint
Gender and age of patient
Circumstances
Risk factors for a disease
Physical Examination
Investigations
Laboratory and
Radiologic test results.
5. Develop a specific differential diagnosis (higher probability causes of chest pain in this patient).
To answer this question you need to know the characteristic pains of different probabilities
Angina:
Mostly felt beneath Sternum
Vague ache to crushing sensation
Radiates to left shoulder, inside left arm, into throat, jaws, epigastrium
Triggered by physical activity, cold air
Usually persists no more than few minutes (5-10 minuts)
Discomfort relieved by rest and Nitroglycerine
Acute myocardial infarction:
Crushing chest pain with or without radiation.
Lasts longer >20 minutes
Not relieved by rest or Nitroglycerine
Diaphoresis, nausea or vomiting
ECG changes
Cardiac enzymes results
Reflux esophagitis:
Esophageal spasm may be severe and centered in the chest although it may also bore to the back.
This pain could also be relieved by nitroglycerin
Worse in supine position
Worse following meals
relieved by antacids or acid blockers
Somatization: One of the most common office complaints is a primary care setting is chest "pain" or discomfort. The complaint often reflects somatization. A point should be made that not all pain is organic; therefore, the physician should pursue psychosocial stresses which may be the initiator of this problem.
Pericarditis. Precardiac, sharp, persistent. Worse in recumbent position Relieved by sitting.
Dissecting aorta. Sharp stabbing pain radiating to back. Asymmetry of pulses.
Chest wall Lesions
Musculo-skeletal injury:
Muscular skeletal pain often is localized along with point tenderness.
Sometimes it mimics pleuritic pain during inspiration.
Pneumothorax: Pain is sudden in onset, localized, sharp, worse on deep breathing and coughing. Associated with shortness of breath.
Pleuritis/pneumonia Pain is sudden in onset, localized, sharp, worse on deep breathing and coughing. Associated with productive cough, fever and chills.
6. What is your diagnosis: Why?
Our primary working diagnosis should be Angina:
Repeated episodes of "heaviness" or chest discomfort during the previous 6 months.
The discomfort seems to be brought on by exertion or eating, is relieved by rest and is localized to the center of the chest.
Age, gender and risk factors support the diagnosis along with the characteristics of the complaint.
We will keep in mind the possibility for Reflux esophagitis and Somatization:( His business is poor and his son is always getting into trouble. Reasons for him having anxiety.) Esophagitis can simulate cardiac pain closely and often can co-exist.
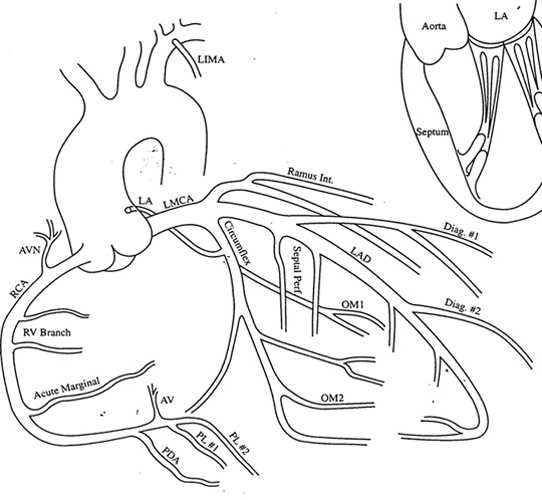
7.Describe the Coronary arterial system.
Right and Left main coronary arteries.
There is some collateral circulation but they mostly behave like end arteries.
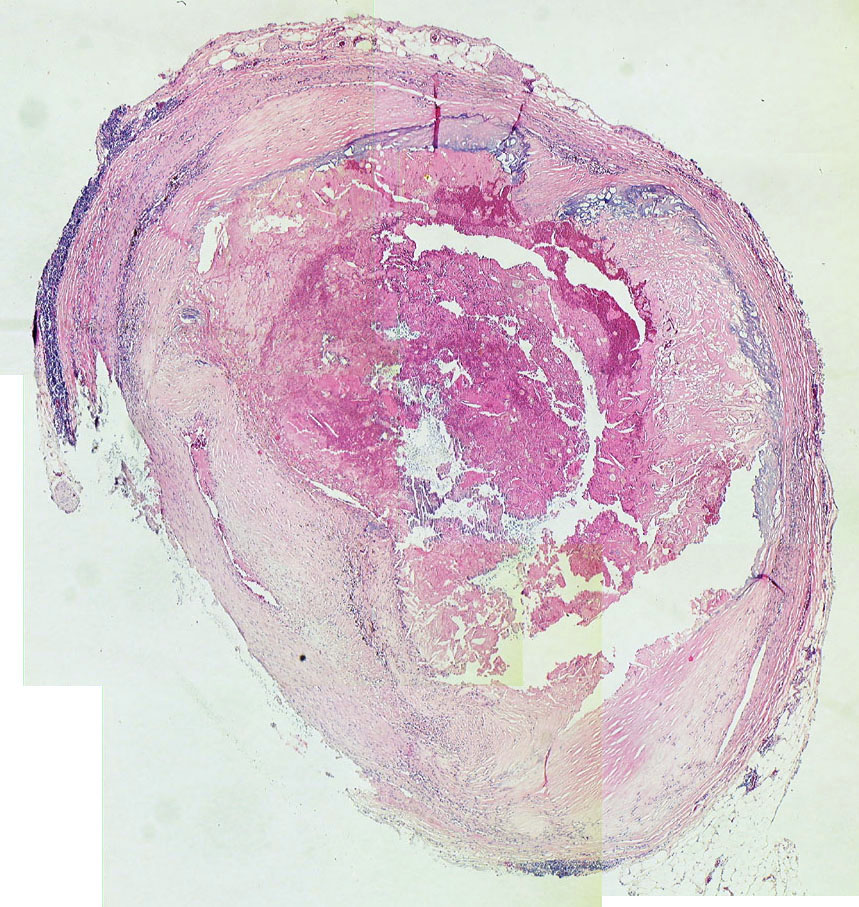
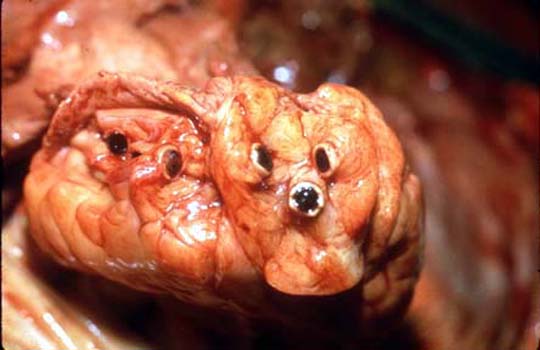
Coronary artery Dissection of the heart (Dr John McNulty)
Coronary artery Dissection of the heart (Dr John McNulty)
Coronary Artery: Branches (Drawing)
8. How is blood flow (oxygen supply) to myocardium regulated and accomplished?
Physiology of coronary flow
Coronary arteries are located on surface of Heart
Myocardium receives blood during distole
Increased myocardial activity requires more blood flow ( exercise, LV hypertrophy)
Direct from ventriclar chamber to myocardium. (small contribution)
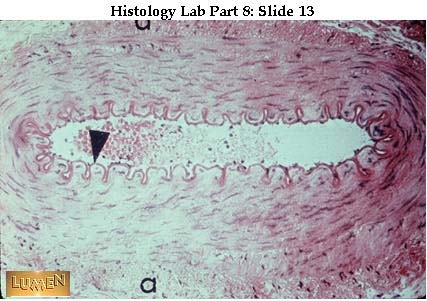
Muscular artery Another medium-sized, muscular artery. (Dr John Clancy)
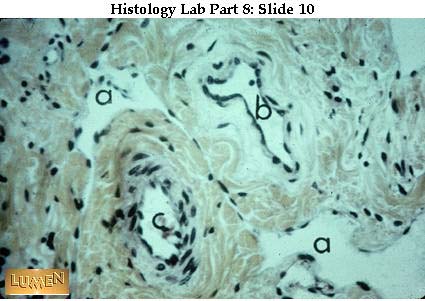
Small blood vessels Small blood vessels, with 3-layered walls. (Dr John Clancy)
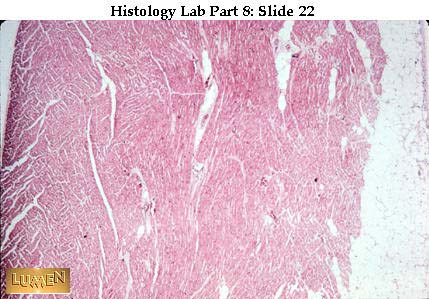
Heart wall The heart wall, like blood vessels in general, has three main layers. (Dr John Clancy)
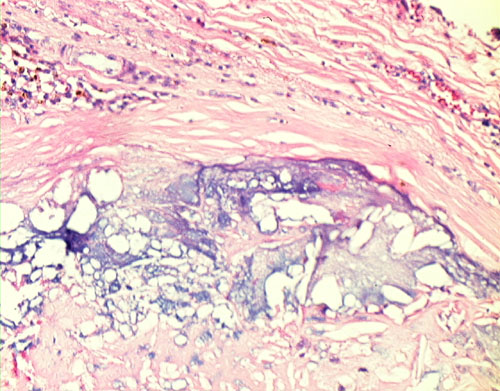
Blood flow to Heart Low power of a Mallory-stained heart, showing two channels that are continuous with the lumen of the left ventricle. (Dr John Clancy)
9. What is the patho-physiology of Myocardial ischemia?
Critical coronary artery obstruction (>70%)
Spasm (Idiopathic, Cocaine)
Increased cardiac work
Calcific Aortic stenosis
Hypertrophic subaortic stenosis
Myocardial O2 demand exceeds the ability of the coronary arteries to supply oxygenated blood.
Coronary sinus blood pH falls/Cellular K loss occurs/EKG abnormalities appear
Ventricular performance deteriorates/LV diastolic pressure rises
Hypoxic metabolites/Discomfort
"The presence of atherosclerosis is not the same as the risk the disease presents. More people die
with atherosclerosis than die of it! "
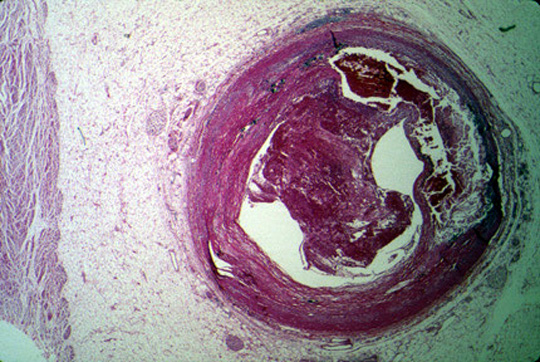
Coronary thrombus: Thrombus coronary artery Gross picture (Dr. Ralph Leischner)
Coronary thrombus: Histo (Dr. Ralph Leischner)
10.What are the risk factors for this disease in this patient?
Hypertension
Diabetes Mellitus
Hypercholesterolemia
Cigarette smoking
Family history of ischemic heart disease
Mr. Solomon has most of these risk factors
11. What is the significance of determining levels of low density (LDL) and high density (HDL) lipoproteins in a patient with increased cholesterol ?
HDL:
Good cholesterol.
Facilitates "reverse cholesterol transport" which helps clear the body of cholesterol
LDL:
Bad cholesterol when it exceeds normal levels.
Most atherogenic lipoprotein
Delivers cholesterol to peripheral tissues cells
Reults in clearance of a low-affinity "scavenger" pathway trigggering cascade of events leading to the development of foam cells
Sensitivity is the proportion of patients with disease that have a positive test.
Specificity is the proportion of patients without the disease that have a negative test.
Positive predictive value is the frequency with which a positive test actually means that the patient has the condition.
Negative predictive value is the frequency with which a negative test actually means that the patient does not have the condition.
The likelihood ratio for a positive test is a ratio of the proportion of patients with the disease who have a positive test (the true positives) to those without the disease who have a positive test (the false positives).
The likelihood ratio for a negative test is the ratio of those with the disease who have a negative test (the false negatives) to those without the disease who have a negative test (the true negatives).
13. In considering Mr. Solomon’s presentation with "pain on my chest" what are the key parts of the history and physical that influence how you develop a differential diagnosis? Qualitatively, what is your impression of the sensitivity and specificity of the historical and physical exam findings?
Mr. Solomon presents with a history of chest pain that is related to exertion and gets better with rest. Chest pain or discomfort is a relatively sensitive question for coronary artery disease but not specific. Mr. Solomon also has a burning chest discomfort that occurs late at night, after large meals, when lying down. More specific details for angina as the diagnosis include the description of the pain as heaviness, the relation to exertion, the relief with rest. The details of the burning discomfort suggest gastro esophageal reflux disease (GERD)
Thus, the specificity of the diagnoses of angina and GERD are increased by the specific historical questions. The physical exam does not add much to either diagnostic possibility. In other words, the increased blood pressure is not particularly sensitive nor specific for the diagnosis of angina. The presence of hypertension, however, increases one’s concern that a patient may have angina given that hypertension is a known risk factor for coronary artery disease .
14 What are the options available for us to make a diagnosis of Angina.
Diagnosis based primarily on history of characteristic pain
Reversible ischemic ECG changes ( ST segment depression, decreased R-wave height, intraventricular or bundle branch conduction disturbances, ventricular extra systoles)
Characteristic relief of discomfort with sub-lingual Nitroglycerin
Exercise stress ECG testing:
Response of ECG to graded exercise
Ischemic response supports Angina
With chest pain specificity 70%: sensitivity 90% in men
Negative test is a reliable indicator of no disease.
Monitors the electrical system to see if there is something wrong with plumbing.
Sensitivity 68%, Specificity 77%
Low sensitivity in submaximal HR
High false positive in females
Enhancing stress test by looking at myovardial perfusion with Thallium
Coronary angiography
Documents the extent of anatomic coronary artery occlusion
Obstruction is physiologically significant when the luminal diameter is reduced >70%
15. What supplemental testing, if any, would you want in addition to the history, physical, and laboratory studies that are listed?
We need to consider Exercise test and Coronary angiogram
It would be reasonable to obtain an exercise test and, depending on the result of that test, proceed with a cardiac catheterization.
One could easily argue, however, given the multiple risk factors and the high prior probability of coronary artery disease, that a negative exercise test may well be considered a false negative and one would go ahead with a Coronary Angiogram anyway. If that is one’ reasoning, then the exercise test would be a waste of time and money.
16. The characteristics of a patient determine how one interprets data obtained from that person. For example, a positive HIV test on a cloistered nun who has never had any sexual contact, blood exposure or other risk is almost certainly a false positive. In Mr. Solomon’s case, what characteristics, or risk factors, make you think it is likely that he has the diagnosis you consider most likely. Given these characteristics, is there any point in supplemental diagnostic testing for Mr. Solomon? Would you believe a negative or positive test? Should be proceed directly to the "gold standard"?
Mr. Solomon is a male smoker with hypertension, hypercholestrolemia, obesity, and a family history of coronary artery disease. The historical data and the risk factors make the prior probability so high that Mr. Solomon has angina, going directly to cardiac catheterization may well be the most reasonable course if one’s goal is to prove that the chest discomfort is angina and related to coronary artery disease.
If Mr. Solomon is averse to invasive testing, a treadmill test might be useful to get a sense of the severity of the coronary artery disease. (i.e. if he drops his pressure with exercise then one would be concerned about left main obstruction and argue more forcefully about the need for a catheterization) and as therapeutic maneuver (e.g., if Mr. Solomon does not have EKG changes until he reaches a high double product, one could consider beginning a gentle exercise program as part of his therapeutic regimen.)
17. What drug therapy would you consider prescribing to control his symptoms?
Strategy (Revisit Pathophysiology to plan a therapeutic option)
Widen this frame for better visualization
Decrease Myocardial Oxygen demand/Coronary artery vasodilatation:
Sublingual nitroglycerine
Organic nitrates are excellent drugs for the treatment of stable angina. The
organic nitrates (R-O-NO2) combine with cysteine (R-SH) in the vessel wall to form a
nitrosothiol that releases nitric oxide (NO). The organic nitrates decrease ventricular
wall stress (oxygen demand) by reducing both preload and after load {wall stress = (P x r)/
(2 x wall thickness)} This results from a primary action on venous capacitance vessels
with a more minor effect on arterioles. Organic nitrates may also exert favorable effects
on oxygen supply. The reduced ventricular pressure during both diastole and systole will
decrease extra vascular coronary resistance (compressive forces). Organic nitrates also
dilate collateral vessels and will cause a small dilation of stenotic coronary arteries
when the stenosis is eccentric.
Dramatic relief within 1.5 to 3 minutes
Dose may be repeated after 5 minutes three times if there is no relief
Patient should carry the tablets always
Drug looses potency/ prescribe small amounts frequently
Long-acting nitrates
If sublingual nitroglycerine worked well but Mr. Solomon wanted something that
prevented his attacks then you could consider switching to a nitroglycerine patch, or
isosorbide dinitrate. Continuous nitrate therapy is not recommended due to the depletion
of cysteine in the vascular smooth muscle and the development of tolerance. A nitrate-free
interval of at least 8 hours is recommended between repeated doses.
Protection against Myocardial Ischemia
Beta-blockers and or calcium channel blockers.
If organic nitrate therapy alone was inadequate to control Mr. Solomon’s angina, then the combination of an organic nitrate and beta-blocker or an organic nitrate with a calcium channel antagonist (verapamil, diltiazem, long acting dihydrophyridine derivative) would provide greater protection against ischemia. Triple therapy consisting of an organic nitrate, beta-blocker and calcium channel blocker might also be considered. The short acting dihydropyridine derivatives (nifedipine) have been shown to increase mortality in patients with coronary artery disease and should not be prescribed.
Beta-blockers block sympathetic stimulation of the heart (reduce Systolic pressure, heart rate, contractility, cardiac output) and reduce myocardial O2 demand.
Calcium channel blockers are vasodilators and are useful when angina is due to spasm or associated with Hypertension.
18. What would you consider to modify Mr. Solomon’s risk factors ?
Alter risk factors
Smoking: Start smoking cessation programs
Hypertension: Anti-hypertensive medication to lower blood pressure (specific agents yet to be covered in the therapeutics lectures-defer)
Hypercholesterolemia: An HMG-CoA reductase inhibitor to lower cholesterol
HMG-CoA reductase inhibitors block the rate limiting enzyme for the synthesis of
cholesterol. Serum cholesterol levels fall not only from a reduced synthetic rate but from
an up-regulation of LDL receptors in hepatocytes and an increased rate of LDL catabolism
from the circulating pool. The HMG-CoA inhibitors (lovastatin, simvastatin,
pravastatin),
have been shown in clinical trials to reduce the rate of progression of coronary
artherosclerotic lesion and to increase the frequency of regression. These agents have
also been shown to reduce the risk of death due to coronary artery disease and risk of
nonfatal myocardial infarction. The goal of this therapy (combined with dietary
restrictions) is to reduce serum cholesterol to <190 mg/dL.
19. What drug therapy would you consider to prevent further progression of obstruction to Coronary arteries ?
Prevent Coronary thrombosis: Aspirin
Since aspirin reduces the risk of heart attack (coronary thrombosis) in patients
with coronary artery disease there is a strong indication for daily aspirin (160 mg/day)
therapy. Aspirin causes irreversible inhibition of platelet cyclooxygenase, decreased
thromboxane A2 production and decreased platelet aggregation. Then aspirin is given as
prophylactic therapy to reduce the risk of intracoronary thrombosis and would probably
have little effect on Mr. Solomon’s angina.
20. What options do we have to relieve mechanical obstruction of Coronary arteries ?
Angioplasty:
Involves insertion of a balloon tipped catheter into an artery at the site of partial obstruction
Inflation of the balloon can rupture the intima and media and dramatically dilate the obstruction
It is an alternative to bypass surgery in a patient with suitable anatomic lesions
Stents can be placed can be placed to reduce reocclusion
Coronary Artery Bypass Surgery
Venous graft
Internal mammary artery graft
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}