Pleural effusion
Arcot J Chandrasekhar, M.D.
Objectives:
- What is pleural effusion
- Various types of effusion and the mechanisms by which fluids accumulate in the pleural space
- Imaging criteria for pleural effusion
- Different appearances of pleural effusion
- Differential for complete opacification of one hemi thorax
- Recognition and significance of loculation
- When to order lateral decubitus
- How to differentiate etiology of pleural effusion
- Role of ultrasound for pleural tap
- Role of CT in thoracentesis
- How to read a CXR with pleural effusion
- How to determine the etiology of pleural effusion
What is pleural effusion?
- Normal pleural space is lined by thin film of fluid. Visceral and parietal pleura are in opposition and glide over each other during respiration.
- When excess fluid accumulates in pleural space, it is called pleural effusion.
- Note pleural effusion on left (yellow arrow) in the adjacent CXR.

What are the types of fluid that can accumulate in pleural space?
- Transudate
- Exudate
- Pus
- Blood
- Chyle
- Cholesterol
- Urine
Cholesterol effusion from a patient with rheumatoid arthritis is shown.
Radiologically they all look similar and cannot be distinguished in plain CXR.

What are the mechanisms by which fluid accumulates in pleural space?
- Transudate: Due to hydrostatic pressure changes as in CHF, cirrhosis and hypoalbuminemia.
- Exudate: Due to inflammation of pleura as in malignancy, rheumatoid arthritis, etc.
- Pus: Empyema from infections.
- Blood: Trauma.
- Chyle: From rupture of thoracic duct.
- Urine: Urinothorax in hydronephrosis.
What are the imaging criteria for pleural effusion in CXR?
Imaging criteria are:- Homogenous density
- Density in dependent portion
- Upright: Costophrenic angle in PA view
- Lateral view: Anterior and posterior portions of gutter
- Lateral decubitus position: Along sides
- Supine position: Along posteriorly, giving diffuse haziness on the side of effusion
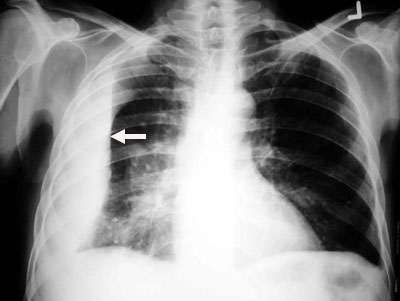
- Silhouette of upper limit of density
- Upper margin high in axilla in PA view (yellow arrows)
- Upper margin high anteriorly and posteriorly in lateral view
- This is just an illusion
- Loss of silhouette. In the images below note lack of identifiable left diaphragm before and visible diaphragm after clearance of fluid (Silhouette sign principle)
- Mediastinal shift



Before thoracentesis
Left diaphragm is not identifiable
After thoracentesis
Left diaphragm is seen clearly.
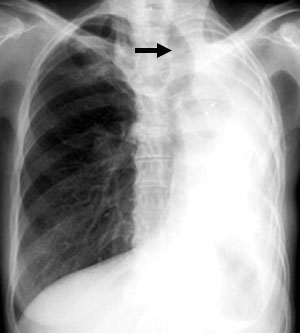
How do you differentiate complete opacification of one hemi thorax in CXR? Unilateral white out of thorax.
Consider:
- Massive pleural effusion
- Complete atelectasis or surgical resection of lung
Mediastinum is shifted to the opposite side with effusion and pulled to same side with atelectasis. Hemi thorax is larger with effusion and smaller with atelectasis. There are other reasons for loss of unilateral lung volume, but for now remember atelectasis and resection.

 t
tMassive effusion on left
-
Mediastinal shift to opposite side
-
Larger hemithorax
Atelectasis of left lung
-
Mediastinum pulled towards atelectasis
-
Smaller hemithorax
What are the different appearances of pleural effusion?
- Massive: Often due to malignancy.
- Unilateral VS bilateral: In CHF effusions are bilateral and more on right.
- Sub pulmonic: Most effusions start like this and can be easily missed.
- Loculated: This type of effusion is empyema unless proven otherwise.
- Supine position: ICU patients cannot sit up and the effusion layers posteriorly.
- Lateral decubitus position
Unilateral haziness
Supine film on left. Note uniform haziness of right hemi thorax.
Upright film on right is now showing sub pulmonic effusion

How do you recognize loculated effusion? What is the significance?
- Loculation should be considered when a density is considered to be fluid and does not correspond to anatomical location of fissures. Of course loculation can occur within fissures.
- It is not in the gravity dependant location.
Note in the upright film on right you are able to see the diaphragm medially, indicating that the fluid is not in the dependent portion.
Empyemas loculate.
Consider all loculated effusions as empyema unless proven otherwise.
When will you order lateral decubitus film?
Lateral decubitus film is obtained:
- To confirm pleural effusion as with small or sub pulmonic effusions
- Occasionally to evaluate underlying lung
Most of the time it is ordered unnecessarily with no additional benefit in large effusions.
Note in the film on right shows the findings of sub pulmonic effusion. The costophrenic angle (black arrow head) is blunted and displaced medially. The distance between the stomach bubble and diaphragm has increased (Black arrow). In the lateral decubitus film fluid layers along the ribs (white arrow heads).

What are the other imaging procedures of value in the evaluation of pleural effusion?
- Ultrasound:
- Ideal for localizing, loculated or small effusions for thoracentesis.
- This can be done at the bedside.
- Debris or septations may be seen in hemothorax or empyema.
- Pleural masses may be seen.
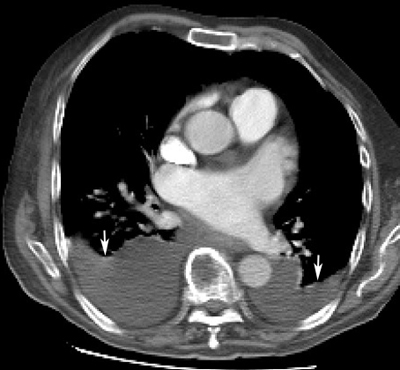
- CT scan can detect pleural masses not evident in chest x-ray. It can detect underlying lung lesions not evident in chest x-ray. CT can also guide placement of tubes into pleural space for drainage.
How does radiological procedures help in thoracentesis?
You do not need any radiological assistance to tap most of the effusions. Obtain radiological assistance to tap:
- With small effusions
- Loculated effusions
Ultrasound is the preferred method for localization of fluid and a needle can be passed through the probe. It can also be done at the bedside if necessary. CT guided tap is equally effective, except it is not useful as bedside procedure.
- that it is a homogenous density
- where it is layering? is it in basal position ? is it loculated
- does the upper margin slat up towards axilla (meniscus sign)
- position of the mediastinum
How do you determine the etiology of effusion from chest x-ray?
Radiologically you cannot distinguish transudate, exudate, blood or pus. It's mainly the associated findings suggest the etiology. Let me give a few scenarios:
Bilateral: consider transudative effusions first. You will need clinical information.
- Congestive heart failure
- Cirrhosis
- Nephrotic syndrome
- Kwashiorkor (hypo proteinemia)
Bilateral effusions with cardiomegaly: Congestive heart failure
Bilateral pleural effusions associated with ascites in a alcoholic: Cirrhosis
Unilateral: most of them are exudative
- Malignancy (primary, secondary, lymphoma etc)
- Infections (tuberculosis, empyemas etc)
- auto immune disease (Rheumatoid arthritis etc)
- trauma
Massive unilateral effusion: Malignancy
Pleural effusion with apical infiltrates: Tuberculosis
Pleural effusion with nodes or mass or lytic bone lesions: Malignancy
Loculated effusions are empyemas
Pleural effusion with a missing breast suggesting resection for cancer : Malignancy
Pleural effusion following chest trauma: Hemothorax
In patients with mediastinal lymphoma : Chylothorax
Unique etiologies for left sided effusions
- pericarditis
- dissecting aneurysm
- rupture esophagus
- acute pancreatitis
Unique etiologies for right sided effusions
- Liver abscess