This module is meant for advanced learner.
Radiological criteria
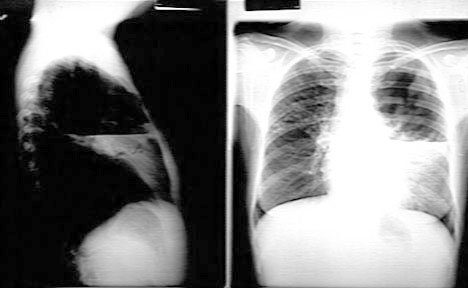
Hole in lung with a wall, lumen and contents. Focus of
increased density whose central portion has been replaced by air.
Following characteristics help in differential diagnosis.
Number
Multiple bilateral cavities would raise suspicion for either bronchogenous or
hematogenous process. Hematogenous lesions usually have sharp margins because they are located in the interstitium. Bronchogenous cavities , the margins are shaggy.
- Bronchogenous
- Aspiration lung abscess
- Coccidiomycosis, Tuberculosis
- Bronchiectasis
- Hematogenous
- Septic emboli
- Metastatic lesions
- Vasculitis (Wegners)
Single cavity
- Primary lung cancer
- Post traumatic lung cyst
- Many other diseases
Size
- A large cavity encompassing the entire lobe or lung should raise suspicion for gangrene of lung.
Location
-
Classical locations for aspiration lung abscess are superior segment of
lower lobes and axillary sub segments of anterior and posterior segments of upper lobes.
- Tuberculous cavities are common in superior segments of upper and lower lobes.
- When a
cavity in anterior segment is encountered, a strong suspicion for lung cancer should be
raised. TB and aspiration lung abscess are rare in anterior segments. Cancer lung can
occur in any segment.
Wall Thickness
-
Thick
walls are seen in
- Lung abscess
- Necrotizing squamous cell lung cancer
- Wegners granulomatosis
- Blastomycosis
- Thin walled cavities Extremely
thin walled cavities are seen in
Lining of wall
The lining of wall is irregular and nodular in cancer
lung or shaggy in lung abscess . The appearance is akin to stalactites and
stalagmites.
Contents
-
Most common cause for air
fluid level is lung abscess. Air fluid levels can rarely be seen in malignancy and in
tuberculous cavities from rupture of Rasmussen's aneurysm.
- A fungous
ball should make you consider Aspergillosis. Blood clot and fibrin ball will have the same appearance.
- Floating Water Lily: I have never seen this. The collapsed
membrane of a ruptured echynococcal cyst, floats giving this
appearance
Associated Features
- Ipsilateral lymph nodes or lytic lesions of bone is seen with malignancy.
- Adjacent thickening of pleura should raise suspicion for fungous ball.
Evolution of lesion
Many times review of old films to assess the evolution of the
radiological appearance of the lesion extremely helpful. Examples
- Infected bullae
- Aspergilloma
- Sub acute necrotizing aspergillosis
- Bleeding from Rasmussen's aneurysm in a tuberculous cavity
Etiology
Cavity can be encountered in practically most lung diseases.
Common diseases and their characteristics
Not all of the cavities you see in CXR are due to lung disease. Be aware of cavities in other locations projecting in
CXR.
- Empyema
- Mediastinum
- Abscess
- Esophagus
- Colon
- Hernia
- Chest wall
- Biliary ectasia
- Colon interposition
Comprehension of the above principles.
- Rationale for multiple bilateral cavities.
- Why does reactivation Tb occurs in superior segments?
- Why does aspiration lung abscess occur in the superior segment
of lower lobes?
- What is the criteria for thick and thin wall ?
- What is the pathogenesis of stalactites and stalagmites?
- What is crescentic sign?
- How do you differentiate between aspergilloma and sub acute
necrotizing aspergillosis?
- Does the location of cavity in a density have diagnostic
significance?
- What is open negative Tb?
- In metastatic disease, when do you get thin walled cavities and
when do you get thick walled cavities?
- How do you distinguish loculated empyema from lung abscess?
Self evaluation
Are you ready to see whether you have learned the subject. Remember not all the rules apply in each case. I am going to show you images. Come up with your differential and then check to see what it turned out to be. You are OK as long as you had it in your differential.
Contact: A.J Chandrasekhar
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}