Pleural Effusion
Physical Findings
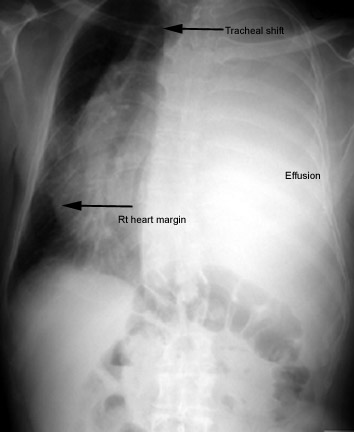
- Mediastinum is in midline
to start with and gradually gets shifted to opposite site as the pleural pressure becomes
positive.
- Chest Expansion decreases on the side of effusion due to
decreased ventilation.
- Resonance is dull and flat to percussion. Dullness is most in
posterior base in erect position. Flatness is recognized by tapping the chest with flat of
your hand. Traube's space will be obliterated on left sided effusions.
- Breath Sounds are decreased since the ventilation to that
hemithorax is decreased. Fluid is a good conductor of sound. If there is underlying
consolidation a good bronchial breathing will be heard over the effusion. In massive
effusions with completely atelectic lung and patent airways one can also hear bronchial
breathing over the effusion.
- Voice Transmission decreases and follows breath sound
characteristics. Egophony is noted
along the upper margin of the fluid. This is probably due to a thin film of fluid
separating pleural space.
- Adventitious Sounds: None
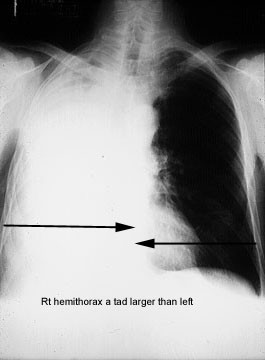
- Hemithorax
size is larger due to loss of negative pressure in
pleural space.
- Effort of Ventilation: Respiratory rate increases and use of
accessory muscles can be recognized.
- Effect on Function: Can lead to central cyanosis.
Focused Exam
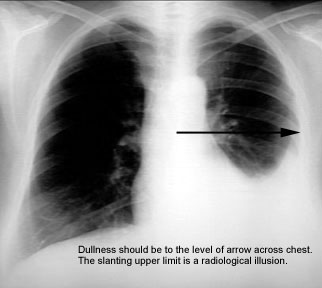
Upper Limit of Fluid can be recognized by:
- Percussion
- Scratch test
- Egophony
The upper limit of dullness should be horizontal
across the hemithorax.
- Shifting Dullness
- Try to elicit shifting dullness. In prone position the previously dull pleural
gutter will become resonant as the fluid shifts and lung floats up. Shifting dullness is
demonstrable with ease when there is hydropneumothorax.
- Diaphragmatic Function
- Ipsilateral diaphragmatic function is decreased and can become paradoxical in
massive effusions.
- Chest Wall Edema
- Chest wall edema is recognizable in empyemas.
- Chest Wall Warmth
- Chest wall increased warmth is recognizable in empyema.
- Clubbing
- Clubbing is associated with malignant effusions and empyemas.
- Exceptions
- Size of hemithorax is smaller in negative pressure induced
pleural effusion.
Mediastinal
shift to the same side of effusion occurs in negative pressure induced
effusion and in lung cancer with endobronchial lesion and atelectasis.
{kind=link}
{kind=link}
{kind=link}
{kind=link}