Anatomical Principles
One should have a clear understanding of anatomy of the respiratory system to perform a proper physical exam. Some of the important anatomical details are outlined below. For details review the link provided to Dr. McNulty's lesson on Thorax by clicking on anatomic principles.
In the surface anatomy exercise we arbitrarily divide the thorax into various spaces and create lines. Localization of abnormal finding is achieved and described using the ribs, interspaces, spaces, and lines.
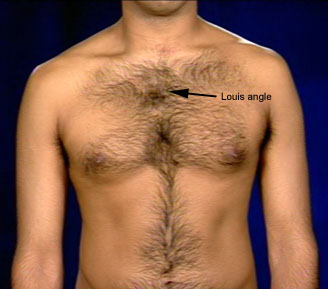
Left Lung: At angle of Louis, follow the outer margin of heart to 6th rib in mid-clavicular line.
Appreciate that apex of lung is just under the skin easily palpable in the supraclavicular space.
Pancoast tumor and TB occur at this site. Hence, the apex of lungs should be routinely examined.
Transverse fissure can be drawn by drawing a line from 5th rib in mid-axillary line to 4th rib anteriorly.
Once the fissures are drawn over the outline of lungs, one can easily recognize the surface anatomy of lobes of lungs. One can then appreciate the importance of examining the patient all around the chest to cover the lobes. Most of lower lobe is in back, upper lobe is in front and all of middle lobe is in front. In the axilla all of the three lobes can be seen.
Sternal angle separates superior from inferior Mediastinum. The inferior Mediastinum is divided into anterior, middle and posterior compartments. The space in front of heart is anterior Mediastinum and behind is posterior Mediastinum. Heart itself defines the middle Mediastinum. The posterior Mediastinum is divided into paravertebral and prevertebral space. Superior Mediastinum extends into the neck and is called cervico-Mediastinal space.
It is important to know the structures in each compartment. In the differential of masses in the Mediastinum one uses this knowledge.
{kind=link}