
|
|
Pathology |
The etiology of sarcoidosis is not known, but there is evidence that the pathologic findings are the result of an immunologic problem. Because of this, it is hypothesized that unknown antigens, either nonself or self, initiate sarcoidosis.
Initially acute inflammation fails to degrade the antigens and then nonspecific chronic inflammation ensues. Lymphocytes and mononuclear phagocytes are attracted to the inflammed area, and in addition, mononuclear phagocytes migrate from the blood to the tissue where they mature into macrophages and phagocytize the antigens in an attempt to neutralize them. These cells are important in the formation of noncaseating granulomas, the histologic hallmark of sarcoidosis.
T-cell lymphocytes are markedly increased in areas of active granulomatous disease, and the ratio of T-helper cells to T-suppressor cells is markedly increased. This is the opposite of the circulating blood where the number of T-cells is reduced and the ratio of T-helper cells to T-suppressor cells is decreased. This exaggerated T-cell activity indicates an altered immune response.
The etiology of the altered T-cell response is not known, but inherited or acquired alteration of immune response genes may be an important factor or the antigen may selectively affect the T-cell arm of the immune response.
A granuloma consists of a central collection of modified mononuclear phagocytes which are called epithelioid cells. Epithelioid cells are derived from macrophages. As macrophages mature to epithelioid cells, they gain secretory and bactericidal capabilities but lose some phagocytic capability. Morphologically epithelioid cells are large, polygonal and have an eliptical nucleus which contains fine chromatin and 1-2 nucleoli. The cytoplasm can be light or dark.
There are often giant cells in the central part of the granuloma. Giant cells are a conglomeration of epithelioid cells which share the same cytoplasm and have multiple nuclei. At first most have randomly distributed nuclei (foreign body type giant cell) but later the nuclei are arranged in the periphery (Langhans type giant cell). The central epithelioid and giant cells are surrounded by a rim of lymphocytes, mostly T-helper cells. Lymphocytes are small, oval, basophilic cells with little cytoplasm.
| SUBPLEURAL GRANULOMA IN LUNG | LANGHANS' GIANT CELL |
|---|---|
|
|
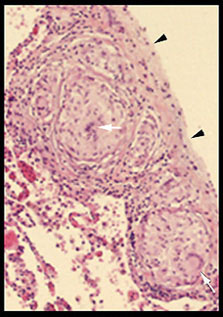
These granulomas are in a typical position, adjacent to the pleura (arrowheads). Note giant cells (arrows) within central collections of epithelioid cells and the encircling rim of lymphocytes. |
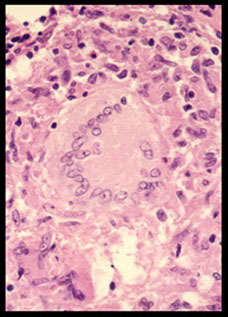
A Langhans' giant cell in the central part of this granuloma is surrounded by epithelioid cells . Note peripherally arranged nuclei in giant cell. |
Early in the formation of a granuloma there may be no surrounding lymphocytes. This is called a naked granuloma.
Several types of cytoplasmic inclusion bodies can accompany granulomatous inflammation including: laminated calcific Schaumann bodies, stellate asteroid bodies, and small oval brown Hamasaki-Weseberg bodies. These inclusion bodies are common in sarcoidosis but are nonspecific.
| CYTOPLASMIC INCLUSION BODY | NAKED GRANULOMA |
|---|---|
|
|
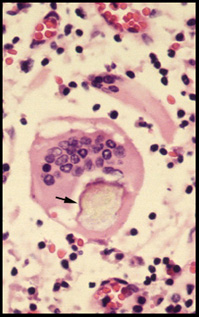
This cytoplasmic Schaumann body (arrow) is common in sarcoidosis but is nonspecific. |
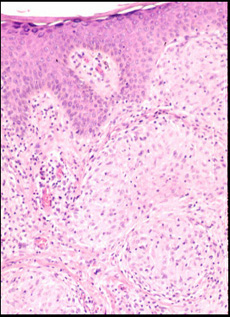
These young granulomas (arrows) in the skin have no surrounding rim of mononuclear cells and are called naked granulomas. |
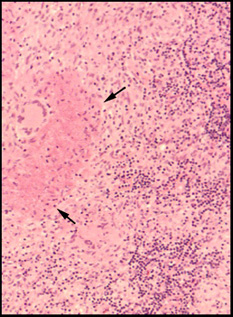
Sarcoidosis is characterized by noncaseating granulomas. These are different than the caseating granulomas produced by other diseases, especially tuberculosis. Caseous necrosis is destruction of cells which are converted to amorphous greyish debris located centrally in granulomas. The term caseous ( L. caseus, cheese) refers to the gross appearance of caseous necrosis which resembles clumped, friable cheese.
| CASEOUS NECROSIS | M. tuberculosis BACILLI |
|---|---|
|
|
Cellular destruction in this tuberculous granuloma appears as clumped debris (arrows). This type of necrosis does not occur in sarcoidosis. |
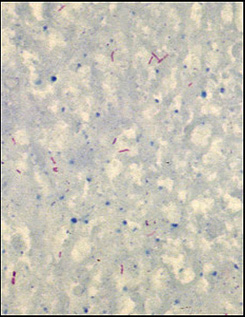
Caseous necrosis is most common in tuberculosis, but Gram negative, acid fast bacilli must be identified to make the diagnosis, as in this patient. |
Damage to tissues and organs is due to the mass affect of granulomas on the anatomy and not to the release of mediators that damage cells.
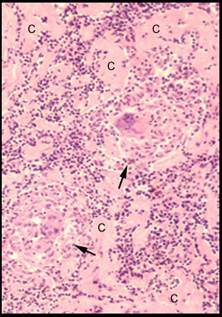
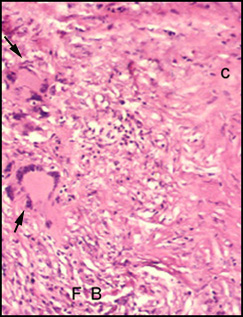
Ganulomas can resolve spontaneously or following steroid therapy. Resolution can be complete, can leave an insignificant fibrous scar, or when there is chronic active disease, can cause more extensive tissue damage and fibrosis which results in permanent organ dysfunction. In these cases fibroblasts proliferate and produce collagen. Granulomas become enclosed by fibrous rims and later replaced by collagenous fibrous tissue.
| EARLY COLLAGEN FORMATION | MORE ADVANCED COLLAGENOUS FIBROSIS |
|---|---|
|
|
Extracellular collagen (C) is being produced by fibroblasts which are difficult to see at this magnification. |
Elongated fibroblasts (FB) with more extensive collagenous fibrous tissue (C). Giant cells (arrows) |


| Terrence C.Demos, M.D. |
Last Updated: March 14, 1996 Created: March 1, 1996 |