What are the useful imaging modalities to investigate cholecystitis?
- US
- HIDA
- CT
- Four views of abdomen
Indicate the utility of each imaging procedure and when you would select each one:
Ultrasound
- It should be the first imaging modality used when suspecting cholecystitis.
- It's non-invasive, fast, easily tolerable by the patient, and reliable in the hands of an experienced operator.
- It may also be difficult to detect stones in the neck of the gallbladder and cystic duct since the valves of Heister typically show echogenicity with strong shadows mimicking calculi.
HIDA Scan
- The HIDA scan should be used when ultrasound is equivocal.
- Intravenous technetium labeled hepatic iminodiacetic acid (HIDA) is taken up by the hepatocytes and excreted into the bile.
- After 30-60 minutes, the scan will show (excretion of isotope) the flow of bile through the biliary tree including common bile duct, cystic duct, and gallbladder.
- HIDA scans can be falsely positive when the gallbladder does not fill in the absence of cholecystitis. These situations include severe liver disease, patients on total parenteral nutrition, hyperbilirubinemia, alcohol and opiate abuse.
CT:
- CT has a secondary role in evaluating the biliary tree with the availability and accuracy of ultrasound.
- However, it is best employed when ultrasound is difficult due to obesity or when complications such as perforation or abscess formation are suspected.
- It can also be used when findings are confusing on ultrasound exam.
- Computed tomography can accurately identify gallstones and gallbladder wall edema.
Image Atlas of Cholecystitis
What are the imaging findings of cholecystitis in four views abdomen?
- Acute cholecystitis is associated with gallstones in approximately 95% of cases, thus it is possible to see gallstones on plain radiograph. (Only 20% of gallstones, however, contain sufficient calcium to be seen on a plain radiograph).
- The duodenum and/or hepatic flexure of the colon may show an ileus from the resulting inflammation of the adjacent gallbladder.
- Very rarely gas may be seen in the biliary tree.
- In two-thirds of cases, the plain radiograph is completely normal or may show mild dilation of small and large bowel.
- In emphysematous cholecystitis air can be recognized in the gall bladder and gall bladder wall.
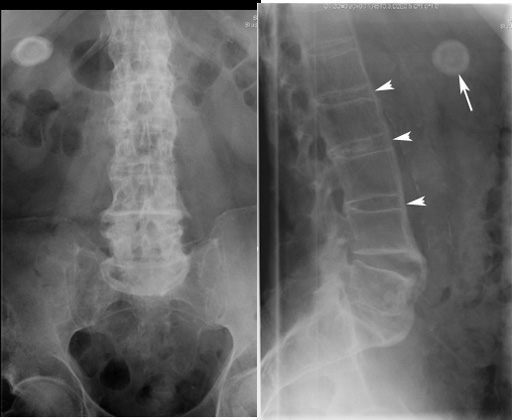
Plain film
Gallstone in a patient with ankylosing spondylitis
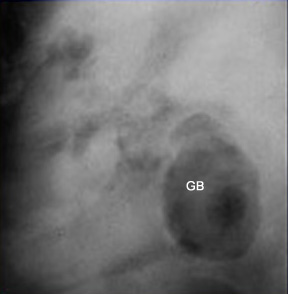
Emphysematous cholecystitis
Air in the lumen of gallbladder
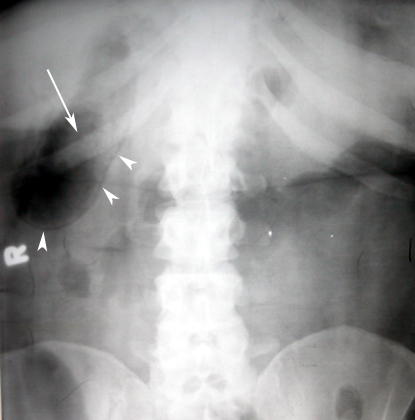
Emphysematous Cholecystitis
Radiograph showing:
- Arrow points to air within the lumen of GB.
- Arrowheads point to air in the GB wall.

What are the imaging findings of acute cholecystitis in ultrasound abdomen?
Ultrasound findings:
- Thick gallbladder wall - greater than 3 mm
- Stones present in gallbladder
- Pericholecystic fluid
- Sonographic Murphy's sign - tenderness over the gallbladder from the ultrasound transducer
- Emphysematous cholecystitis:
- Air in gallbladder
- Air in wall of gallbladder
- Acalculus cholecystitis:
- Thickened gallbladder wall
- No stones seen
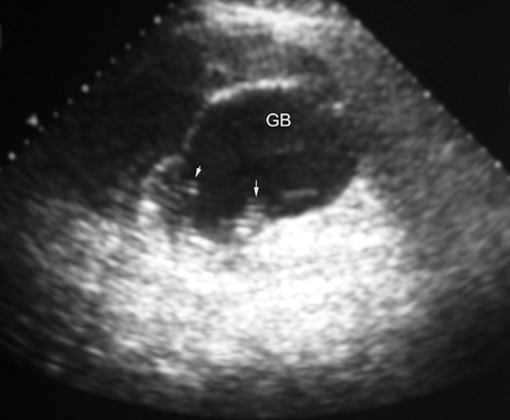
Gallstones - Acute cholecystitis
US findings:
- Thick GB wall
- Stones in GB
- Absence of echoes posterior to the calculi "Shadowing"
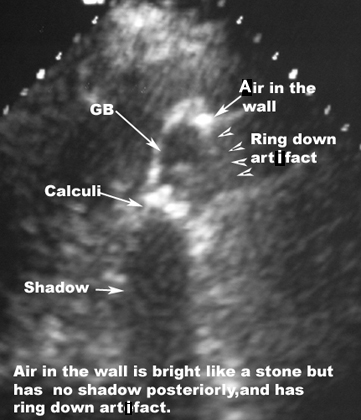
Acute Emphysematous Cholecystitis
Ultrasound showing:
- Thick wall of GB
- Stones in GB
- Air in GB
- Air in wall of GB is bright like a stone but has no shadow posteriorly, and has ring down artifact.
Emphysematous Cholecystitis
Arrows point to ring down artifacts from air in the wall and lumen of GB.
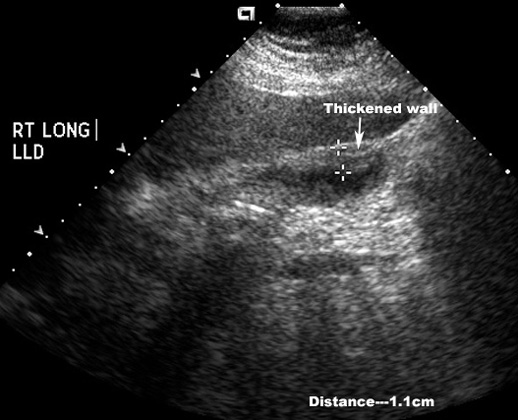
Acute acalculous Cholecystitis
US Finding:
Thickened gallbladder wall
What are the imaging findings of acute cholecystitis in radionucleotide cholescintigraphy (HIDA Scan)?
- No isotope accumulation is visible in the gallbladder indicating obstruction of the cystic duct.
- Normal excretion is seen into the duodenum.
- This is diagnostic for cholecystitis and is usually done if the ultrasound study shows no stones.
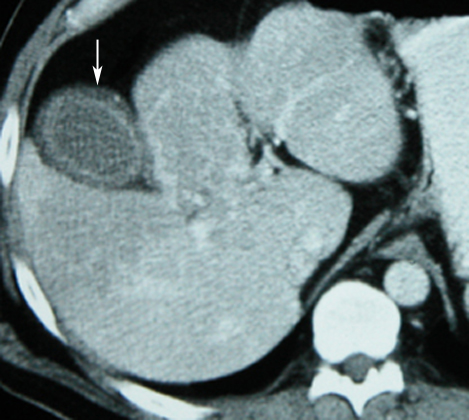
What are the imaging findings of acute cholecystitis in CT abdomen?
The most common findings on CT are:
- gallstones
- wall thickening (>3 mm)
- pericholecystic fluid
- inflammation in the pericholecystic fat
- subserosal edema seen by poor definition of the gallbladder/liver wall interface
- Air in GB: Emphysematous cholecystitis
- Air in GB wall
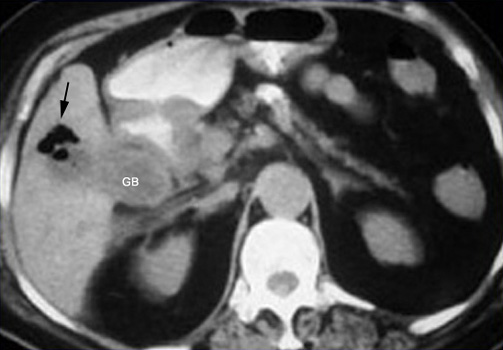
Emphysematous cholecystitis
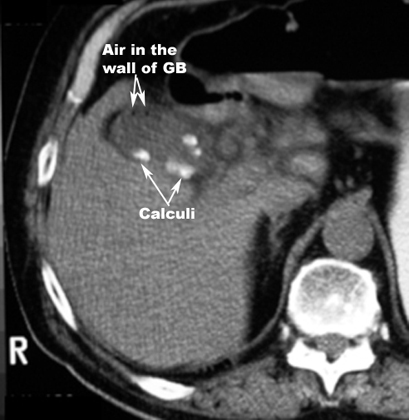
Emphysematous Cholecystitis
CT Findings:
- Air in the wall of GB
- GB calculi
Sensitivity and specificity of each:
- Ultrasound: The sensitivity of ultrasound in the detection of acute cholecystitis is 95% and the specificity is 78-80%. The combination of gallstones and a positive sonographic Murphy's sign has a positive predictive value for acute cholecystitis of as high as 90-96%.
- Nuclear Medicine: The HIDA scan has a sensitivity and specificity of approximately 95%. The negative predictive value of a normal exam (i.e.: visualization of the gallbladder within 1 hour) in excluding acute cholecystitis is greater than 99%.
- CT: The sensitivity and specificity of CT scans for predicting acute cholecystitis has been reported to be greater than 95%.
What is the procedure sequence/ diagnostic algorithm in a suspected case of acute cholecystitis?
- If the H&P suggests acute cholecystitis and an ultrasound should be ordered right away. Ultrasonography is a rapid, safe and low cost.
- Unfortunately, patients with acute abdominal disease frequently have excessive gas that interferes with careful and detailed sonograhic evaluation of the abdominal organs.
- Overlying gas, bone, and fat do not impair imaging with CT.
- Consider a CT if the patient is obese or you suspect an abscess or possible perforation.
- Consider a HIDA scan if ultrasound is negative or indeterminate. For example, if there was a sonographic Murphy's sign and gallbladder edema without gallstones, a HIDA scan may still be positive in acalculous cholecystitis.
- When evaluating for stones, options include plain abdominal radiographs (S/S = 64/68), ultrasound (S/S = 91/97), and CT (S/S = 79/99).
- When evaluating for acute cholecystitis options include ultrasound (S/S = 91/79), color velocity imaging and power Doppler ultrasound (S/S = 96/100), and radionuclide scanning (HIDA scan) metanalysis (S/S = 97/90).
- For common duct obstruction, options include ultrasound (S/S = 95/93 in one study, and 63/94 in another), CT (S/S = 98/98 in one study and 71/97 in another).