Pancreatic Cancer
Pathology
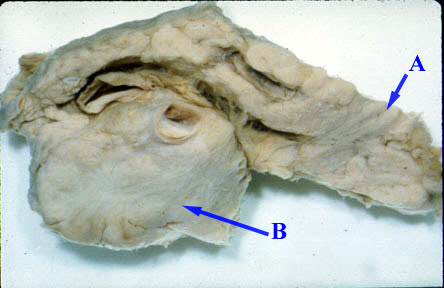
- The neoplasm and the extensive fibrosis replaces most of the normal pancreas.
- Tumor can be located anywhere in pancreas.
- The neoplasm, in the head of the pancreas, can compress the common bile duct causing an extra hepatic obstruction.
- Dilatation of intra hepatic bile ducts, common bile ducts [CBD] and gallbladder [Courvoisier GB]
- Cancer in the tail of pancreas may obstruct the splenic vein or cause mass effect on adjacent structures.
- The neoplasm, in the head of the pancreas, can compress the common bile duct causing an extra hepatic obstruction.
The pancreas is bisected along its longitudinal axis revealing a large adenocarcinoma (B) of the head. (A) is the tail of pancreas which is normal.
What are the useful imaging procedures in the evaluation of cancer pancreas?
- CT scan is ideal to evaluate tumor and to stage.
- US and Nuclear Medicine studies are primarily useful to demonstrate biliary obstruction.
- Retrograde cholangiopancreatography
- MRCP: MR cholangiopancreatography
Indicate when you would select each procedure.
- Abdominal ultrasound:
- The initial study in patients who present with jaundice is usually abdominal ultrasonography (US).
- Dilated bile ducts or the presence of a mass in the head of the pancreas suggest the presence of a pancreatic mass/tumor.
- Intestinal gas often interferes with US evaluation of entire abdomen
- CT scan:
- CT may be particularly useful in patients who are not jaundiced, and in those in whom intestinal gas interferes with US.
- CT may reveal bile and pancreatic duct dilation, a mass lesion within the pancreas, and evidence of extra pancreatic spread including liver or lymph node metastases and ascites thus useful for staging.
- ERCP: Retrograde cholangiopancreatography:
- ERCP is most useful for patients in whom CT or US does not reveal a mass lesion within the pancreas, and in those in whom the differential diagnosis includes chronic pancreatitis.
- Findings suggestive of a tumor/mass include super-impassable strictures, obstruction of the common bile and pancreatic ducts (the "double duct" sign), a pancreatic duct stricture in excess of 1 cm in length, pancreatic duct obstruction, and the absence of changes suggestive of chronic pancreatitis.
- Endoscopic ultrasound (EUS):
- There has been variable accuracy using EUS in diagnosing pancreatic masses.
- It is very operator dependent, and as a result its value varies widely with locally available expertise.
- MRI:
- MRI can visualize both the bile and pancreatic ducts, and may be particularly useful in patients in whom attempted ERCP is either totally unsuccessful or provides incomplete information because of pancreatic duct obstruction.
What are the imaging findings of cancer pancreas?
- Mass
- Biliary tract obstruction when the carcinoma is in the head.
- Dilatation of intra hepatic bile ducts, common bile ducts [CBD] and gallbladder (Courvoisier GB).
- Cancer in the tail of the pancreas may obstruct the splenic vein or cause mass effect on adjacent structures.
Sensitivity and specificity of each:
| Test | Sensitivity | Specificity |
| Ultrasound | 80 | 90 |
| Endoscopic US | 90 | 90 |
| CT scan | 90 | 95 |
| Retrograde cholangiopancreatography | 90 | 90 |
| MRI scan | 90 | 90 |
Image Atlas for Pancreatic Cancer


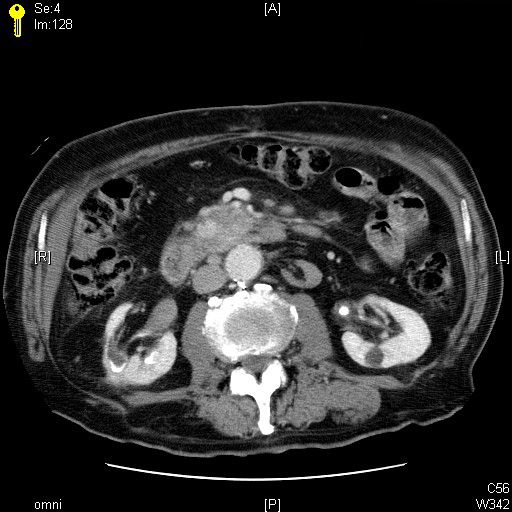
CT scan in a patient with Cancer Pancreas
Black arrowheads points to an irregular mass in the head of the pancreas.
- SMA: Superior mesenteric artery
- SMV: Superior mesenteric vein
- Duo: Duodenal sweep
Carcinoma pancreas
Arrows: Note enhancing mass head of pancreas extending medially into the uncinate process.
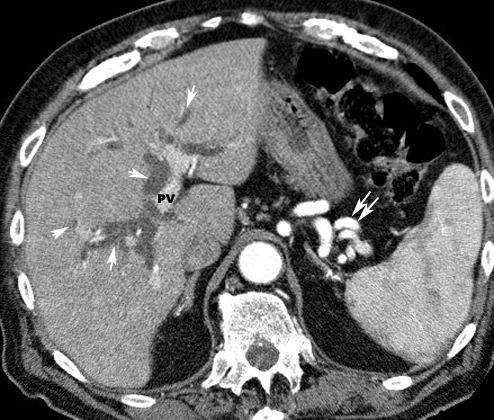
Carcinoma pancreas
Arrows point to dilated intra hepatic bile ducts indicating obstructive jaundice.
Bile ducts are next to contrast filled branches of the portal vein (PV).
Double arrows point to perisplenic varicosities.

CT scan in a patient with obstructive jaundice due to Cancer Pancreas
Dilated common bile duct
DUO: Duodenum
SMV: Superior mesenteric artery
SMV: Superior mesenteric vein
CBD: Common bile duct
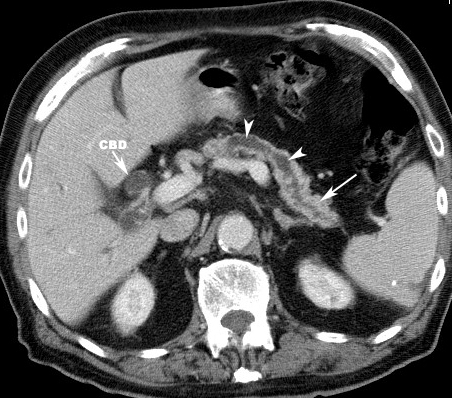
Carcinoma pancreas
- CBD: Dilated common bile duct
- Arrowheads: Dilated pancreatic duct
- Arrow: Tail of pancreas

Carcinoma pancreas
-
GB points to dilated gallbladder
-
Arrowheads point to small cysts in pancreatic head
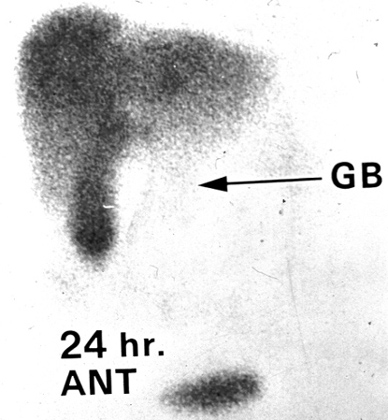
Courvoisier gallbladder
The liver and a distended gallbladder are seen in this nuclear medicine study isotope. However, no excretion of the isotope into the bowel is seen indicating a complete obstruction of the common bile duct.
Isotope has been taken up by the liver parenchyma and with excretion into GB indicating patent cystic duct. But there is no spill into the duodenum which indicates common bile duct obstruction