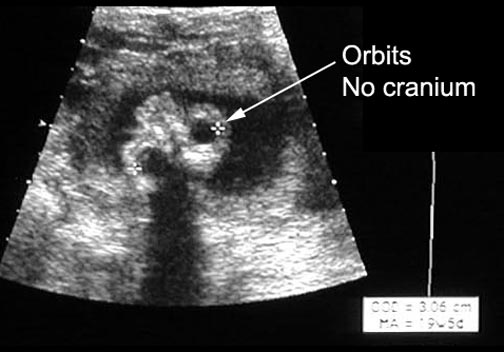
Anencephaly
What is the clinical setting when you will consider anencephaly?
Factors that place a woman at increased risk include:
- Family history of neural tube defects.
- Women with increased risk of neural-tube defects are offered alpha-fetoprotein (AFP) testing as part of a diagnostic work-up.
- Exposure to certain environmental agents: diabetes (hyperglycemia), hyperthermia, drugs and medications (anticonvulsants - valproic acid and carbamazepine), aminopterin, isotretinoin.
- Neural-tube defects as part of a genetic syndrome with known recurrence risk: Meckel-Gruber, Roberts-SC phocomelia, Jarco-Levin, and HARDE Syndromes.
- Individuals who belong to high-risk racial or ethnic groups and/or in high-risk geographic regions: United Kingdom > China, Egypt, India >U.S.
What is the useful imaging modalities in evaluating anencephaly? What is the utility of the procedure, including limitations and accuracy?
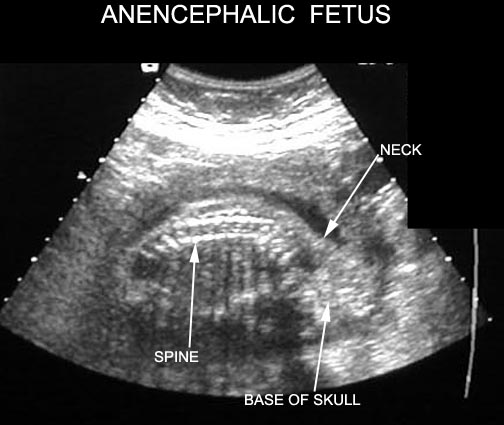
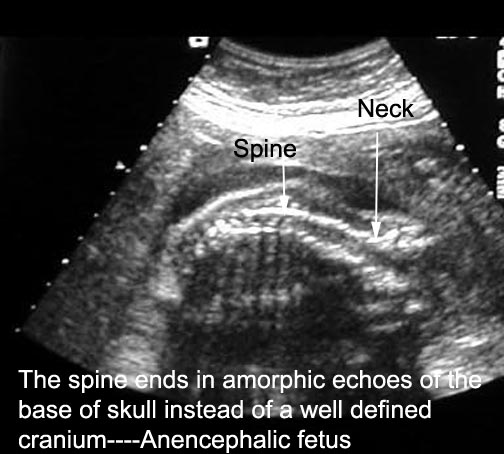
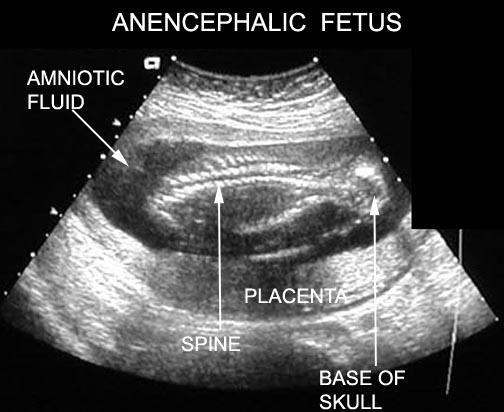
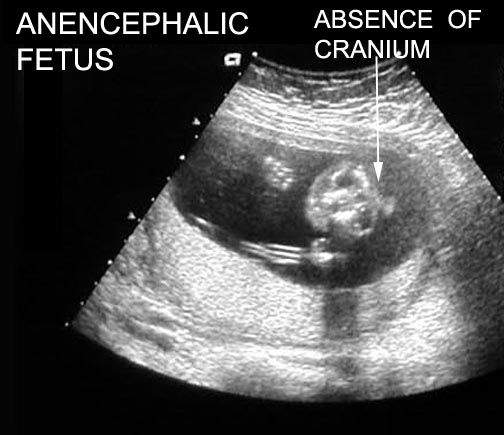
- Ultrasound.
- Anencephaly can theoretically be diagnosed as early as 8 weeks; however, it can be missed in the first trimester.
- There is 100% accuracy in the second trimester for this diagnosis by ultrasound.
- One study showed sonography alone was 97% sensitive and 100% specific in diagnosing an open neural tube defect.
Findings indicative of another neural tube defects:
- Lemon sign: frontal notching. Fetal head looks like a lemon.
- Banana sign: elongated cerebellum.
- Obliteration of the cisterna magna.
- Ventriculomegaly with the lateral ventricle width greater than 10 mm.
- Small bi parietal diameter.