Clinical Considerations: Atypical Clinical Presentation
Case 1
| Perforated appendicitis mimicking
gastroenteritis. A 3 year old boy presented to the emergency room at an outside hospital with a four day history of anorexia, abdominal pain, fever, and a 24 hour history of emesis. A clinical diagnosis of gastroenteritis was made and he was treated with Bactrim. Due to persistent pain, constipation for three days, and new onset of abdominal distention, he was transferred to our hospital for surgical consultation. At this time his abdomen was diffusely tender; positive peritoneal signs were noted on physical examination. Leukocytosis was now present. An abdominal radiograph was obtained, shown below. |
|
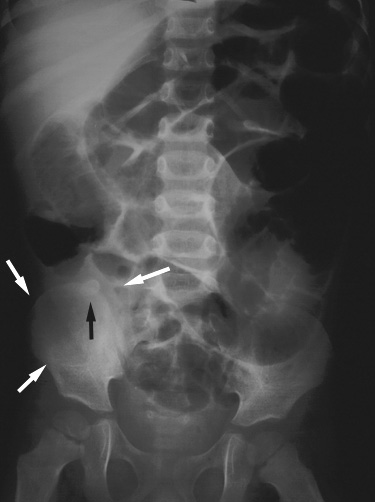
Supine anteroposterior radiograph of the abdomen shows dilated, air-filled small bowel loops with no air in the rectum, consistent with bowel obstruction. There is paucity of gas in the right iliac fossa, most likely due to an abscess (white arrows). A calcified appendicolith (black arrow) overlies the right iliac crest. |
| At laparotomy, 20 cc of frank pus were suctioned from the right lower quadrant periappendiceal abscess, and an appendectomy was performed. |
Related teaching points can also be found in Plain Film Findings
Return to Atypical Clinical Presentation (C)
| Perforated appendicitis mimicking small bowel
obstruction. 4 year old girl presented with a four day history of anorexia, nausea, and vomiting. Physical examination was significant for pain on rectal examination. Plain films, a barium enema, and CT examination were obtained, shown below. |
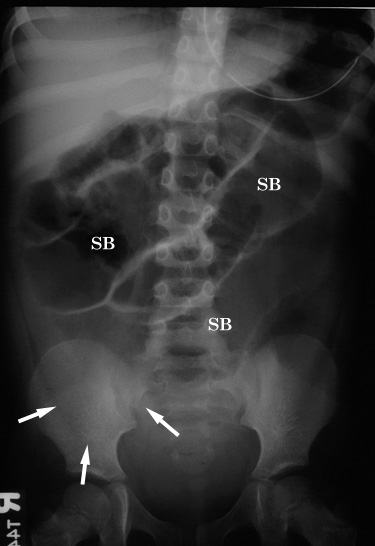 |
Figure 1. Supine abdominal radiograph shows multiple air-filled, dilated small bowel loops (SB) consistent with mechanical small bowel obstruction. Note paucity of bowel gas in the right lower quadrant (arrows) and absence of a calcified appendicolith. |
 |
Figure 2. Right posterior oblique film obtained during single-contrast barium enema shows partial opacification of the appendix (arrows) which is irregular in contour. C = cecum. |
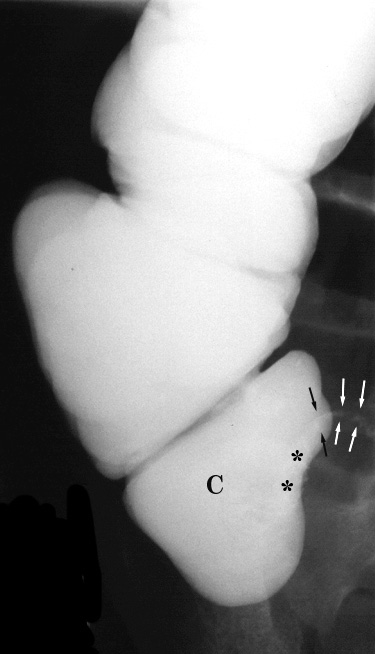 |
Figure 3. Spot compression view of the cecum (C) during single contrast barium enema demonstrates mass effect upon its medial border (*). Note the irregular margins of the partially opacified appendix (arrows). |
 |
Figure 4. Contrast-enhanced CT image of the mid-pelvis shows a midline gas and fluid collection (A) consistent with an abscess. The appendix is not visible. |
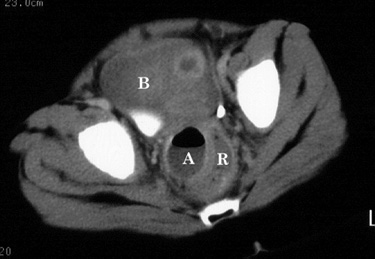 |
Figure 5. CT image at a lower level than Figure 4 shows extension of the abscess (A) deep into the pelvis, contiguous with and causing mass effect on the rectum (R). B = urinary bladder. |
| At surgery, a pelvic abscess resulting from perforated appendicitis was confirmed. |
Related teaching points can also be found in Plain Film Findings
Return to Atypical Clinical Presentation (C)
Return to Barium Enema Findings
Return to CT Findings