|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Problem Orientated Medical Record (POMR)The POMR as initially defined by Lawrence Weed, MD, is the official method of record keeping used at Foster G. McGaw Hospital and its affiliates. Many physicians object to its use for various reasons - it is too cumbersome, inhibits data synthesis, results in lengthy progress notes, etc. However, the proper use of the POMR does just the opposite and results in concise, complete and accurate record keeping. A brief overview of the salient features of the POMR will be helpful. The basic components of the POMR are:
Note: 1, 2 and 3 above must be completed by the admitting physician. DATABASEThe importance of the Data Base is obvious and must include a complete history and physical exam. Many hospitals include certain routine laboratory studies (CBC, SMAC, EKG, chest x-ray, urinalysis, etc.) for each patient admitted. If these are available to the admitting physician, they are to be included in the initial data base along with a history and physical. As additional information is collected it is added to the Data Base. COMPLETE PROBLEM LIST
After the admitting physician performs the history and physical, reviews the basic laboratory data and records the data base, the Problem List is constructed and recorded. The construction of a Problem List is the initial step (for the next step, see number 3 - Initial Plans) of what physicians "really do". That is, once they have seen the patient, physicians think about and define "what is wrong with the patient" or "what are this patient's problems." Problems are either active or inactive (inactive problems are usually prior, resolved medical or surgical illnesses that are still important to be remembered). Dr. Weed had defined an active problem as anything that requires management or further diagnostic workup. Physicians often get caught up in defining Problems and Problem Lists, accusing each other of lumping, splitting, etc. This is unnecessary. Important facts to be noted in constructing a problem list are these:
Resolving problem 2-6 under 1, uremia, allows one daily progress note to be written for that problem and tells an observer reading the patient's chart that all the signs and symptoms in problems 2-6 are related to manifestations of uremia. The date 5/3 tells the observer to see the notes of that day to explain the redefining of the Problem List.
The date 5/9 refers an observer to that date's progress note which will explain why the problem is considered resolved.
Again the date of 5/7 will refer the reader to the progress note for that day which should reveal the result of the renal biopsy.
Example: A female patient who is admitted with upper GI bleeding has not had a pelvic exam in 2 years. A pelvic and Paps are not done on admission because the patient is unstable. The problem list must include a problem that states:
Once the patient is stable and the pelvic exam/Pap smear is done, the problem is resolved.
Example: For an elderly, lonely female who is admitted with a hip fracture and whose physical exam is normal except for the hip and whose answers are positive for every question asked in the review of systems, the physician could list the problems: #1 - Fracture left hip, and #2 - Positive review of systems. Or, recognizing that all these affirmatives may be manifestations of depression, the physician could list #2 - Depression.
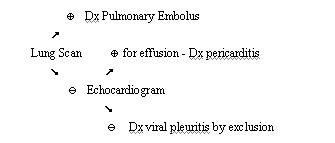
INITIAL PLANSThe next process that a physician undertakes after deciding "what is wrong" is "what to do about what is wrong." This is the initial plan and must be written by the admitting physician after the Problem List is constructed. For each problem defined, a SOAP note must be recorded. The Subjective and the Objective are each a brief review of the abnormalities identified in the history, physical, and initial lab data, which pertain to that particular problem. These need not be lengthy, but simply one or two lines reviewing the pertinent data. The Assessment is a brief but pertinent paragraph describing what the physician thinks about that particular problem. If the problem recorded is a sign or symptom requiring a differential diagnosis, the DD must be recorded in a prioritized manner with a brief statement as to why the physician includes the differential that he or she does. If the problem is a known diagnosis (example - asthma), the physician must include in the Assessment a statement that describes the severity and why the problem has worsened requiring admission to the hospital. The Plan must include three distinct groupings: Diagnostic Plan: The diagnostic plan includes all the diagnostic workup which the admitting physician feels will be necessary. If the Assessment includes the differential diagnosis, then each must be ruled in or ruled out in the diagnostic plan. This may be done by way of a Venn diagram. Consider a 23 year-old female admitted with pleuritic chest pain for which the admitting physician includes pulmonary embolus pericarditis, or viral pleuritis in the differential diagnosis. The diagnostic plan may be as follows: If the problem is a known diagnosis, then the diagnostic plan must include additional workup needed either to further define the problem or to assess the severity of the problem.
DAILY PROGRESS NOTES
FINAL PROGRESS NOTE OR DISCHARGE SUMMARY
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
© Loyola University Chicago Stritch School of Medicine. All rights reserved. |