Auscultation
of lungs help determine the airway and alveolar integrity, ventilation and presence of abnormality.There are two normal breath sounds. Bronchial and vesicular . Breath sounds heard over the tracheobronchial tree are called bronchial breathing and breath sounds heard over the lung tissue are called vesicular breathing. The only place where tracheobronchial trees are close to chest wall without surrounding lung tissue are trachea, right sternoclavicular joints and posterior right interscapular space. These are the sites where bronchial breathing can be normally heard. In all other places there is lung tissue and vesicular breathing is heard.
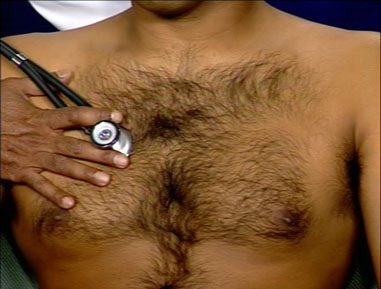
Method of Exam
Use the diaphragm of the stethoscope. Listen to the chest posteriorly, in axilla and front of chest similar to the way lungs were percussed. Follow the same routine, listen to breath sounds from top to bottom and compare sides by alternating corresponding sites. Listen to at least one complete respiratory cycle at each site. First listen with quiet respiration. If breath sounds are inaudible, then have him take deep breaths.
Note the intensity of breath sounds, symmetry, length of inspiration and expiration. Listen for the pause between inspiration, expiration and the quality of pitch of the sound. Compare the intensity of breath sounds between upper and lower chest in upright position. Compare the intensity of breath sounds from dependent to top lung in the decubitus position. Note the presence or absence of adventitious sounds.
Normal
The vesicular breathing is heard over the thorax, lower pitched and softer than bronchial breathing. Expiration is shorter and there is no pause between inspiration and expiration. The intensity of breath sound is higher in bases in erect position and dependent lung in decubitus position.
The breath sounds are symmetrical and louder in intensity in bases compared to apices in erect position. No adventitious sounds are heard.
Abnormal
Intensity of breath sounds, in general, is a good index of ventilation of
the underlying lung. If the intensity increases there is more ventilation and vice versa.
Breath sounds are markedly decreased in emphysema.
Symmetry: If there is asymmetry in intensity, the side where there is decreased intensity is abnormal.
Any form of pleural of pulmonary disease can give rise to decreased intensity.
Bronchial breathing anywhere other than over the trachea, right clavicle or right interscapular space is abnormal. Presence of bronchial breathing would suggest:
In all these conditions, there are no ventilation into alveoli and the sound that is heard originates from bronchi and is transmitted to the chest wall.
Experienced physicians could discriminate between consolidation and cavitation by noting the quality of bronchial breathing. In consolidation, the bronchial breathing is low pitched and sticky and is termed tubular type of bronchial breathing. In cavitary disease, it is high pitched and hollow and is called cavernous breathing. You can simulate this sound by blowing over an empty coke bottle. In tension pneumothorax bronchial breath sounds has a metallic quality and is called amphoric breathing.
Caution:
Example:
{kind=link}
{kind=link}