In 1977, Dr. Mario Rizzetto and associates discovered in Italy, in patients affected by Hepatitis B a new antigen different than surface, core and e systems that they called "delta antigen". (Gut 18:997-1003,1977). This antigen was detected by immunofluorescence in the nuclei of liver cells in patients infected with hepatitis B and looked similar to hepatitis B core antigen. Delta, however was not present in cases positive for core; was not present in cases negative for s antigen and was present in only some cases positive for s antigen. Therefore came the suspicion that the new antigen might belong to a different virus. This hypothesis, tenaciously postulated by Dr. Rizzetto, was confirmed some years later by experimentally infecting chimpanzees and obtaining a new viral particle which was given the name of Hepatitis D Virus (HDV).

--a HBS Ag envelope from hepatitis B virus.
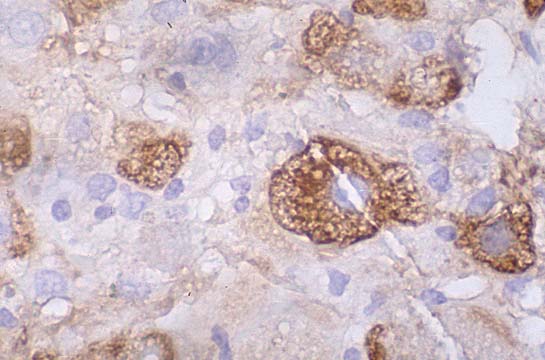
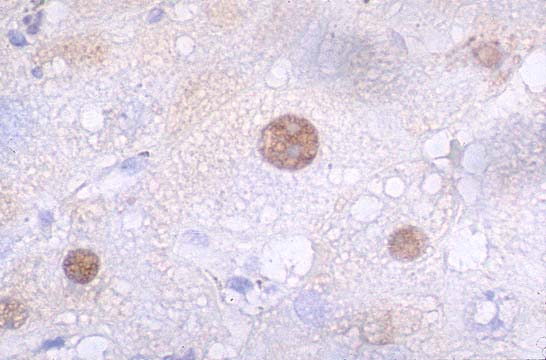
--a delta Antigen predominantly found in the nuclei and in small amounts in the cytoplasm of hepatocytes.
--a single stranded circular RNA, with 1636 bases, a segment of which has a plant viroid sequence and does not encode any protein while another segment is dissimilar and encodes the delta antigen. The virus, therefore, operates with the help of HBV which makes its capsule. It is the only viroid-like agent so far known to infect humans.
Transmission is by blood. Infection may occur simultaneously with Hepatitis B virus (coinfection) or it may be acquired after B (superinfection).In the case of coinfection the patient displays two transaminases peaks, the first apparently due to hepatitis B an the second, which occurs weeks later, due to hepatitis D infection. The acute infection is bifasic.
-- Most cases of coinfection resolve. Only 2.4-4.7% become chronic carriers. This course is apparently due to the fact that HDV seems to suppress HBV replication and does not have optimal conditions for its own replication.
--Most cases (50-70%) of superinfection develop a severe form of acute hepatitis and 90% of them become chronic carriers. This course is due to the fact that the D virus infects hepatocytes heavily colonized by B viruses which provide the D with excellent help for replication. With both infections there is more incidence of fulminant hepatitis and the mortality rate is 5% versus 1% with hepatitis B alone. Hepatitis D does not increase the incidence of extrahepatic disease or hepatocellular carcinoma over hepatitis B infection.
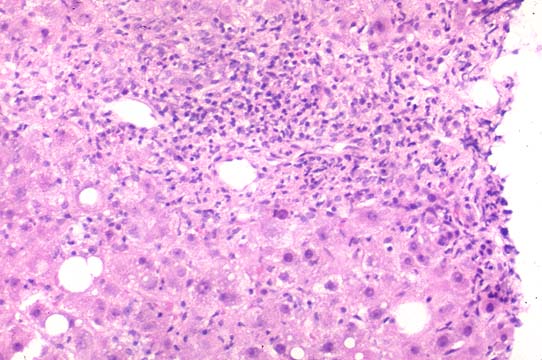
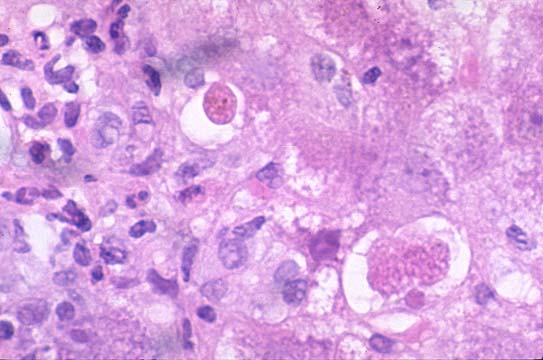
--Delta hepatitis is considered to be the most severe viral hepatitis. In acute forms it produces more fatalities. In chronic forms it produces more cirrhoses even in children. However it has marked geographical variations. While it is very frequent and lethal in the Amazonian basin with peculiar microvesicular fatty infiltration of hepatocyte it is very benign in Greece and south Pacific.
46 year old gentleman presented icteric hepatitis with; Total bilirubin 19.4, ALT 4000, AST 3800, Positive serology for HBV surface antigen, HBV core antigen and HDV antigen. The microsopic picture was that of severe acute hepatitis. A case of coinfection.The patient expired 10 days after this biopsy
It is based on the use of a blocking RIA test for anti-HD antibody. Also available are assays for HDAg, IgM anti-HD, HDV-RNA. In acute resolving infection anti-HD will appear 30-40 days after onset of symptoms and will persist for 1-2 years. In chronic cases the total antibodies (IgM + IgG) will continue to remain high.
All measures that prevent hepatitis B will prevent HDV, including HBV vaccine. Treatment will alpha -interferon is not successful. Liver transplantation is to be considered in fulminant cases. Five year survival after liver transplantation is around 70%. For the fact that HDV has a suppressive effect on HBV replication, the recurrence of accelerated disease after transplantation is less frequent than in hepatitis B alone.