|
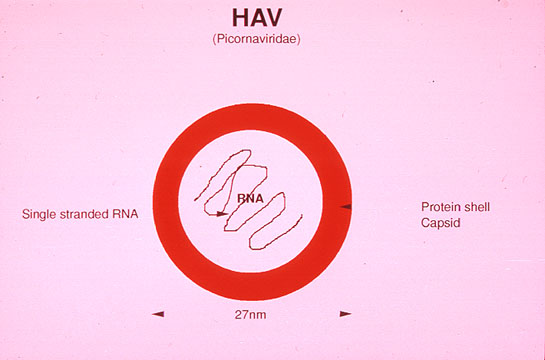
Replication: After entry into the host cell, the virus loses the capsid and the uncoated RNA induces the host cell to produce the viral polyprotein without shutting off the protein synthesis of the cell. Among the viral proteins there is a protease for the synthesis of structural proteins and a polymerase for the replication of viral RNA which becomes rapidly encapsidated into new viruses.
Cultivation in vitro: The virus grows poorly in primate cellular cultures and loses virulence by in vitro passages.
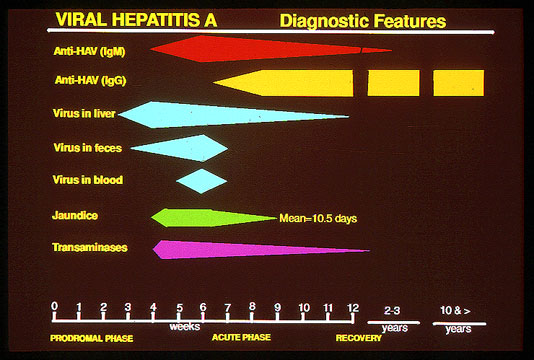
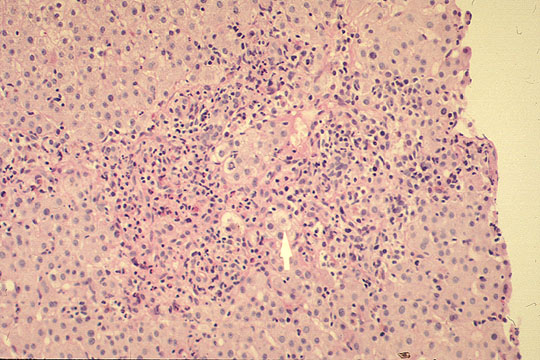
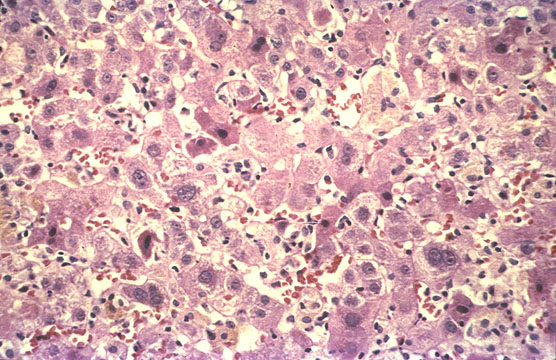
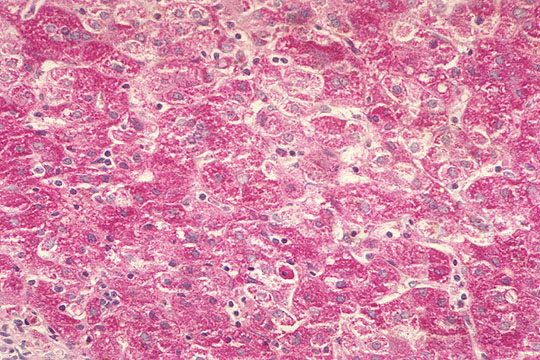
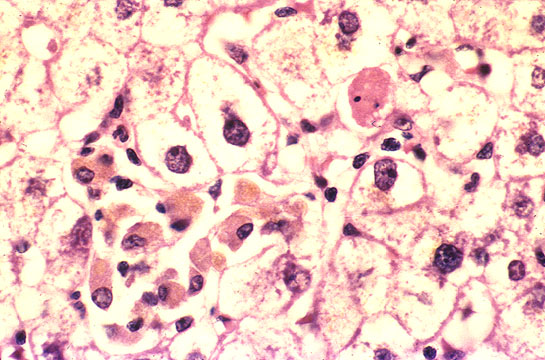
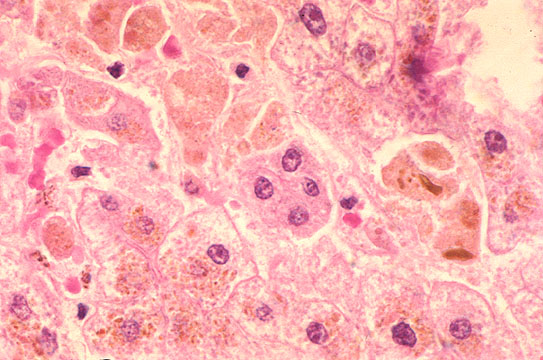
Route of entry and Progress of infection: The virus is acquired by ingestion. It multiplies in the intestine and invades the blood, liver and saliva before any clinical manifestation of the disease appears. This period of incubation lasts an average of 4 (2-6) weeks. The virus disappears soon after the peak of serum transaminase is reached at which time the immune response and the hepatocellular damage start. This indicates that the damage is immunologically mediated. Indeed at this time NK (natural killer) cells, circulating or local in the liver (Pitt cells), are activated. CD8+ cytotoxic T lymphocytes that secrete gamma interferon infiltrate the field.
Clincal features: Most infections occur in children in whom the disease in most cases is either asymptomatic or symptomatic without jaundice. In adults, the infection is more severe with general symptoms malaise and jaundice; however hepatitis A is not very debilitating even in the presence of jaundice. Fever does not go above 39 degrees centigrade. Jaundice lasts for 7-10 days and the whole illness lasts about 4 weeks. Relapses however do occur especially in patients who resume drinking alcohol or exercise and may go on for 6 months. Typically all clincial forms with the exception of the lethal fulminant type resolve with complete liver regeneration without chronicity or long-term carrier state.
CLINICAL FORMS
ASYMPTOMATIC
73% children adults
SYMPTOMATIC WITHOUT JAUNDICE
Gastro-enteric form
SYMPTOMATIC WITH JAUNDICE
65% children adults
RELAPSING
3.8-6.6%. It occurs on an average of 4 weeks after remission and can occur more than once. Relapses may rpesent as any clinical form including fulminant lethal type. Normally it terminates in complete resolution.
CHOLESTATIC
Prolonged clinical course with marked jaundice lasting up to 8 months. Serum bilirubin is 10-20 mg and higher. In spite of this jaundice, the patient feels well and regains. It mimics biliary obstruction, therefore it must be recognized in order to avoid looking for other cholestatic anomalies of the liver. It responds to a short course of oral prednisone.
FULMINANT
It is very rare, 0.5% of cases. Survival with good medical treatment may be 80%. With liver transplantation it may be 55-75% and the graft may become infected with hepatitis A virus but, in general, with a benign resolving clinical form.
EXTRAHEPATIC INVOLVEMENT
Very rare; arthritis, vasculitis, oliguria, urticaria.
VIRAL HEPATITIS A IN PREGNANCY
There is more incidence of fulminant form, however in developed countries pregnant women do like non-pregnant ladies. This indicates that the state of nutrition might make the difference.
CHRONICITY
None
|
|
Pre-exposure
|
A person preparing for travel or to contact an affected individual or a pregnant lady should first check serum IgG level for HAV immunity. If the test is positive, no immunoprophylaxis is necessary. The immunization is achieved with Serum Immunoglobulin (SIG) or with inactivated polio vaccine (the first one marketed by Smith Kline, Beecham Biologicals, Rixensart, Belgium, under the name of Havrix). |
|
Post-exposure
|
Serum immunoglobulin (SIG) must be administered within 2 weeks after exposure in the amount of 0.02 ml/Kg. Antibody level induced by this treatment is low and cannot be measured by standard methods. The main side effect of immunoglobulin injection is considerable soreness in the injection site. The cost is low.
|
|