|
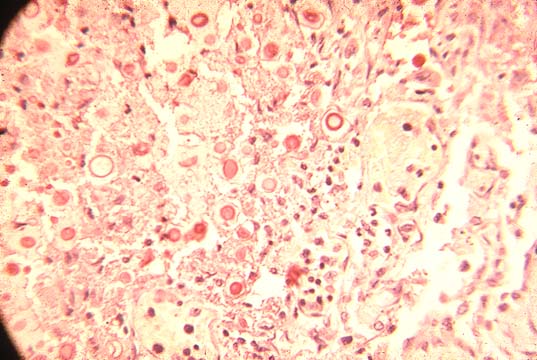
There are numerous bile ductules at the periphery of the portal field. Some are distended and contain inspissated bile. These changes can be seen practically in every portal space.
Contents: Sepsis; Pyogenic liver abscess; Tuberculosis;Mycobacterium avium intracellulare;Bacillus Calmette-Guerin; Leprosy; Brucellosis;Salmonellosis; Tularemia; Listeriosis; Granuloma inguinale; Fungal infections; Siphylis; Leptospirosis; Lime disease;Relapsing fever; Rocky montain spottded fever).
Sepsis
During generalized bacterial infections, septicaemia, although the infection is extrahepatic, the the liver may sustains a damage leading to hepatomegaly and jaundice which may be severe. The retained bile pigment will be seen in the bile canaliculi especially in the centrilobular area and in the periportal bile ductules of Hering. This jaundice was already observed in cases of pneumococcal pneumonia over one century ago. In children and in cases of " septic shock syndrome" due to staphylococcal infection the liver shows commonly canalicular cholestasis with necrosis in the centrilobular area. In cases of other bacterial infections especially those with gram negative bacteria, retained bile is also seen in the bile ductules, ductular cholestasis. The periportal ductules show proliferation and dilatation containing inspissated bile and neutrophils, a process which is not due to obstructing cholangitis because interlobular bile ducts are not involved. The jaundice is due to conjugated hyperbilirubinemia. Serum alkaline phosphatase is elevated. Transaminases are not increased. The pathogenesis is probably that of impairment to the excretion of conjugated bile. Experimentally, bacterial endotoxin reduces bile flow and the excretion of bile, BSP and indocyanine green in the rat.
|
Fig.135-Ductular cholestasis There are numerous bile ductules at the periphery of the portal field. Some are distended and contain inspissated bile. These changes can be seen practically in every portal space. |
Pyogenic liver abcess
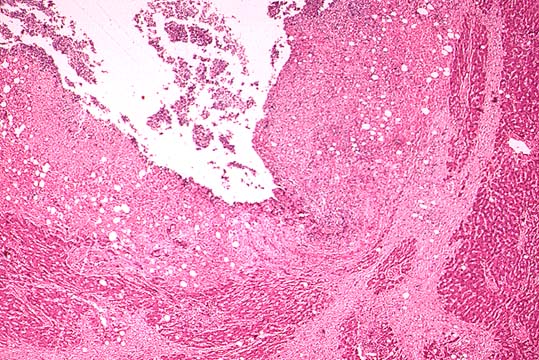
Bacteria colonize the liver by three routs: a)biliary, b)portal, c)hematogenous. Ascending biliary infection accounts for the majority of multiple small liver abscesses. In the pre-antibiotic era the most common source of intra-abdominal infections reaching the liver through the portal circulation was appendicitis. Now it is still observed after pelvic, urinary tract and purulent infections of large intestine, all due to multiple organisms. Clinical symptoms consist of recurrent fever, leukocytosis with or without shoulder tip, pleuritic and right upper quadrant pain. These symptoms may persist for months. The abscess can be discovered by imaging techniques. Treatment consists of drainage and antibacterial therapy. Most cases are now cured with only antibiotics. The present illustration is from a fatal case of liver abscess complicating and acute diverticulitis of the sigmoid colon. The bacteria commonly isolated from pyogenic liver abscesses are E. Coli and enterococci, among the aerobic group and Clostridium perfringens and septicum among the anaerobics.
|
Fig.136-Pyogenic liver abcess Cavity of a large abscess due to diverticulitis of the sigmoid colon apparently present for some time because the cavity is surrounded by a considerably thick fibrous capsule. |
Tuberculosis
It involves the liver most frequently in miliary tuberculosis where it forms multiple granulomas with or without giant cells or caseation necrosis. It is rare to see the organisms in these lesions with acid-fast stains. If the granulomas are numerous the only functional change may be elevation of serum alkaline phosphatase due to the local compression of the liver parenchyma around each single granuloma. TB granulomas in the liver may be very similar to those of sarcoidosis because caseation necrosis is often absent. They however, at difference with sarcoidosis may contain, besides histiocytes and giant cells, a few neutrophilic leukocytes. Because the organisms are rarely seen in TB granulomas of the liver, the histological differential diagnosis with sarcoidosis may be difficult.
|
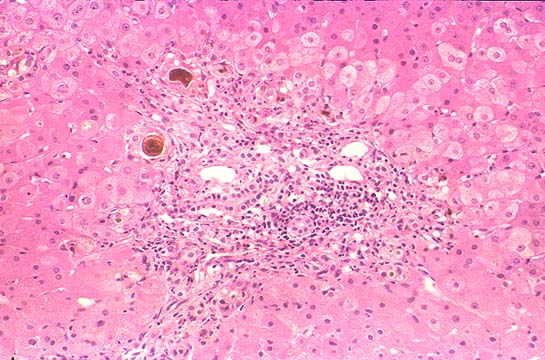
Fig.136-TB granuloma ,early, in the middle of the lobule. On the part of the liver there is only moderate, non-specific portal inflammation and some compression of the liver plates.(H&E stain) | |
|
Fig.137-Same TB granuloma at higher power containing histiocytes and many neutrophils which are a distinguishing feature from non- infectious granulomas. No giant cells nor caseation necrosis at this early stage.(H&E). |
M. Avium intracellulare
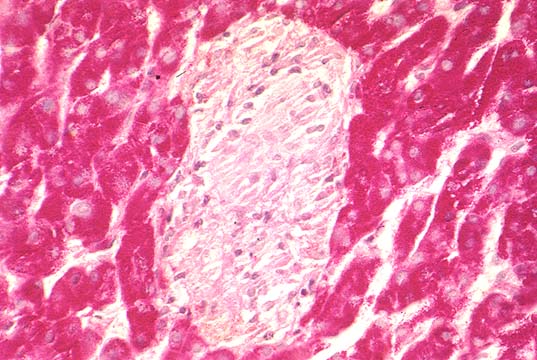
The granulomas are similar to sarcoidosis because they do not have caseation necrosis. The infection is seen in immunosuppressed individuals especially AIDS. The histiocytes of these granulomas contain numerous acid-fast bacilli.
Mycobacterium tuberculosis avium intracellulare |
Fig.138-Granuloma of Mycobacterium tuberculosis avium intracellulare containing only histiocytes. No neutrophils, nor giant cells or caseation necrosis. (PAS stain). | |
|
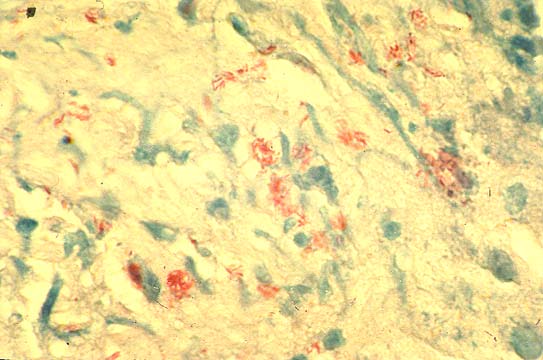
Fig.139-Same granuloma with acid-fast stain. The acid-fast organisms, red, are agglomerated inside histiocytes. |
Bacillus Calmette-Guerin (BCG)
This attenuated bacillus tuberculosis is used for vaccination against Tb and for immunotherapy for malignant neoplasms such as melanoma and urinary bladder tumors. During these procedures it may spread to other organs including the liver where it produces granulomas similar to TB and sarcoidosis. The granulomas will contain acid-fast bacilli.
Leprosy
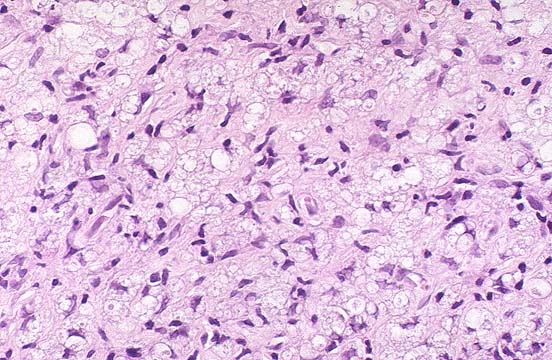
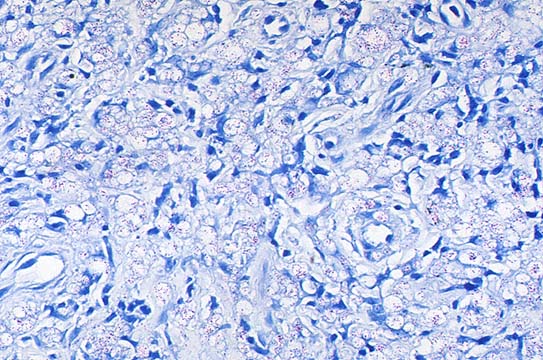
Liver granulomas are observed in the lepromatous form of the disease. They contain acid-fast bacilli and the "lepra histiocyte" which are large histiocyte with clear cytoplasm.
The organisms stain faintly with acid-fast stains, therefore the decoloration step during
the staining procedure must be cut shorter. Hepatic granulomas may be the cause of relapse after an apparent successful therapy.
Lepromatous granuloma with H&E stain. The tissue is composed of histiocytes, some vacuolated, "lepra cells". |
Notice clumps of faintly stained acid-fast bacilli. |
Brucellosis, Salmonellosis, Tularemia, Listeriosis, Granuloma inguinale may all infect the liver where they produce histiocytic granulomas.
|
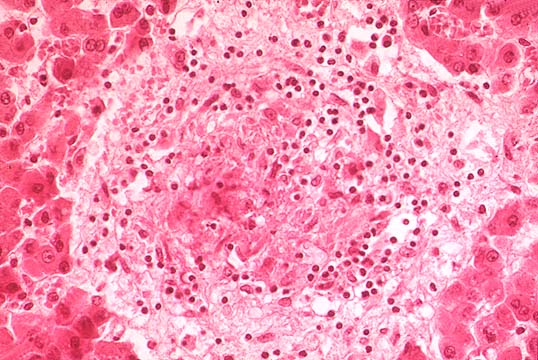
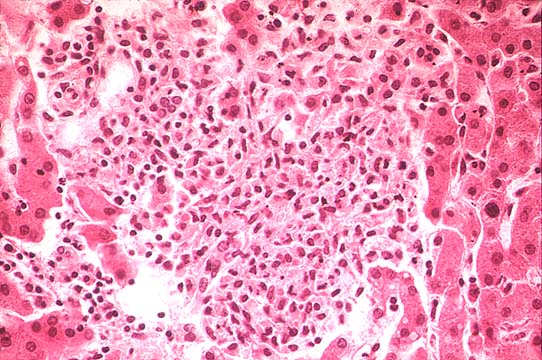
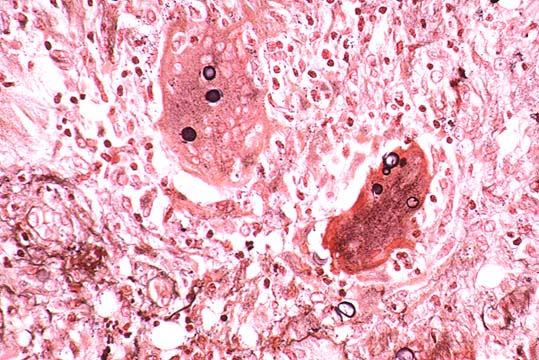
Fig.142-Salmonellosis The illustration shows a granuloma produced by Salmonella typhi, the typhoid nodule, which consists of an intra parenchymal focus of necrosis with histiocytes, some neutrophils an will contain the gram negative organisms. |
Brucellosis in the chronic form will cause similar lesions, sometimes with atypical nuclei of their histiocytes as to mimic Hodgkin’s granulomas especially considering the fact that Hodgkin’s disease lesions in the liver do not have classical Reed cells with mirror-image nuclei but only Sternberg cells with the atypical large dark nuclei.
In Granuloma inguinale foamy macrophages contain Donovan bodies, Donovania granulomatis, which can be seen in the sections with Warthin-Sperry silver stain.
Listeria monocytogenes in the adult may cause granulomas similar to tuberculosis, even with caseation. In neonates the disease is more septic and fatal and produces in the liver numerous micro abscesses resembling miliary TB, therefore the name to the infection of "granulomatosis infantiseptica".
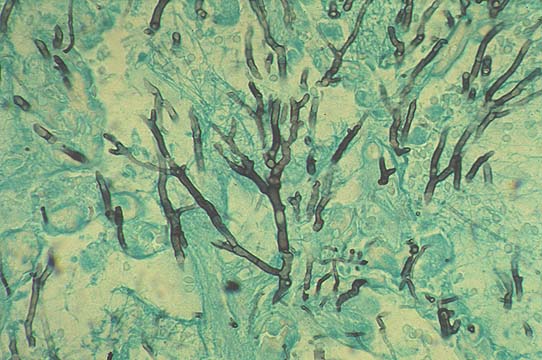
Aspergillosis |
Cryptococcosis |
Blastomycosis |
Coccidiodomycosis |
Syphilis
This historical disease used to produce the "hepar lobatum" in its congenital form due to dissecting fibrosis produced by granulation tissue containing spirochetae pallidae and hepatic granulomas in any form. It is now treatable. Leptospirosis due to the spirochete Leptospira icterohemorrhagica produces the Weil’s syndrome: hemorrhages, jaundice, circulatory collapse, proteinuria, acute liver failure high mortality. The infection is acquire by contact with urine of dogs , pigs , rats, etc. At difference of viral hepatitis liver transaminases are not elevated in the serum. Disorganization of liver cell plates with separation of hepatocytes one from another is a peculiar autopsy finding in this disease a picture often seen in post-mortem changes.
Lyme disease due to the spirochete Borrelia burgdorferi is acquired from Ixodid ticks. The organism injected in the skin produces Erythema chronicum Migrans in the first stage for a couple of months, accompanied with hepatitis, nervous symptoms fatigue, musculoskeletal pain. Brain and cardiac involvement follow in the second stage. The third stage is characterized by arthritis similar to rheumatoid arthritis. The hepatitis is characterized by fatty infiltration, ballooning of hepatocytes, mitotic activity, focal necrosis. Spirochetes are present in the sinusoids. ALT and AST are moderately elevated. Relapsing fever is due to a spirochete Borrelia recurrentis and transmitted by a louse, pediculus humans. It induces recurrent high fever with arthralgia, myalgia, nausea, vomiting petechial hemorrhages of skin and conjunctiva, hepatomegaly and jaundice in the majority of patients. After about 10 days there is resolution by crisis with dangerous circulatory collapse. Another similar acute episode will recur after about 10 days without fever. Fatal cases succumb by hemorrhagic complications, hepatic failure, cardiac failure due to perivascular histiocytic interstitial myocarditis or rupture of the spleen due to splenic abscesses. The liver shows necroinflammatory changes with elevation of serum transaminases and serum bilirubin up to 15mg/100ml. Penicillin, tetracycline and erythromycin are effective treatment.
Rocky Mountain Spotted Fever. It is due to a rickettsia transmitted by ticks. Recorded in Montana, Bitterrot Valley in 1873.The organisms after infection proliferate in endothelial cells of various organs. The clinical syndrome 2 to 14 days after the tick bite starts with fever, malaise, vomiting. On the third day a skin rash appears on the limbs. Later the rash disappears leaving hemorrhagic spots. Jaundice is present in 1/3 of the cases with portal inflammation and presence of rickettsiae in the portal spaces. The organisms can be demonstrated by immunofluorescence. Early treatment with tetracycline, doxycycline and chloramphenicol has lowered the mortality from 23% to 3%,