|
Epithelial damage: swelling, pyknosis, hyperplasia, disorientation, loss of PAS granules. Inflammation: lymphocytes , plasma cell, histiocytes. Confined to portal area. Invasion of ductal epithelium by lymphocyte. Granuloma formation. |
li-11-5 PRIMARY BILIARY CIRRHOSIS by Dr E. Orfei
Definition:
Progressive destruction of interlobular and septal bile ducts with non-purulent inflammatory reaction.
Etiology:
The cause is not known. It is probably an autoimmune disease because:
-It is often associated with other autoimmune diseases:
-The inflammatory reaction consists mainly of T-lymphocytes.
-95% of affected patients have disease-specific anti-mitochondrial antibodies (AMA) which cross-react with gram-negative bacteria.
-Presence of immune complexes.
Pathogenesis.
In this disorder suppressor T lymphocytes (TS) are reduced. Cytotoxic lymphocytes(TC) recognize HLA class II antigens and other antigens on bile-duct epithelial cells. They attack and destroy the epithelial cells. The mechanism is unknown. The defective immunoregulation may be initiated by an infectious agent, such as a virus, attacking the bile duct epithelium. A duct epithelium of other organs such as pancreas and lachrymal glands may be attacked in the same manner.
Pathology.
The disease begins with damage of small interlobular and septal bile ducts. Their epithelial cells become swollen with pyknotic nuclei, irregular in size and shape. Their basement membranes are interrupted. The ducts rupture. They become surrounded by a dense aggregate of mononuclear inflammatory cells: mainly T lymphocytes with plasma cells, histiocytes and eosinophils. The bile ducts are destroyed. Bile ductules proliferate. Histiocytes may form granulomas. Cases with granulomas have less ducal damage and a better prognosis (Lee, Gastronterology, 81:983, 1981). The bile duct destruction is followed by portal and periportal fibrosis with disappearance of bile ducts. Cirrhosis is finally established. The lesion is conventionally divided into four stages:
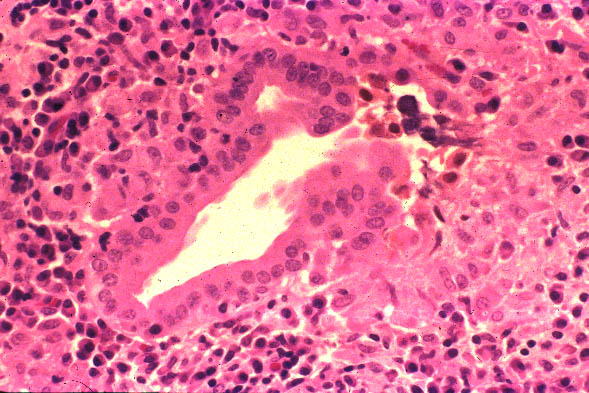
STAGE I - FLORID. Bile duct damage with inflammatory reaction.
STAGE II - PERIPORTAL. Vanished bile ducts, portal and periportal inflammation and ductular proliferation.
STAGE III - FIBROSIS. Portal fibrosis, portal, periportal and bridging, typically without bile ducts.
STAGE IV - CIRRHOSIS.
The characteristic of this disease is its focal character. The anatomical changes are found at the same time in different stages in different portal areas.
STAGE I
|
Epithelial damage: swelling, pyknosis, hyperplasia, disorientation, loss of PAS granules. Inflammation: lymphocytes , plasma cell, histiocytes. Confined to portal area. Invasion of ductal epithelium by lymphocyte. Granuloma formation. |
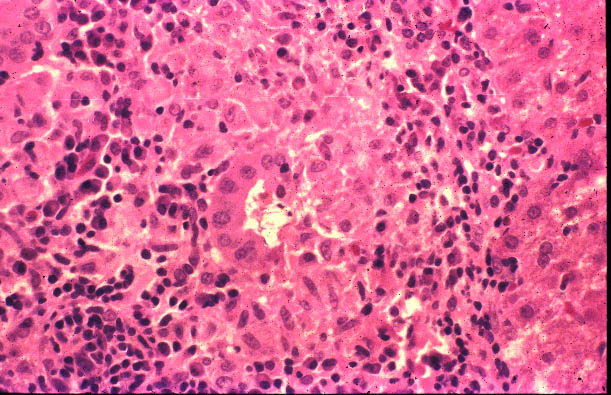 Fig.
11-5-2 Histiocytic granuloma. Fig.
11-5-2 Histiocytic granuloma.
This is a septal space, larger than a portal area. I contains a bile duct, mononuclear inflammatory reaction with mainly lymphocytes and an agglomerate of histiocytes forming a granuloma. Sometimes the histiocytes may form multinucleated giant cells and the lesion may like sarcoidosis. |
STAGE II
|
Disappearance of bile ducts. This portal area shows only an artery, no portal bile duct. The inflammatory reaction is still present and becoming periportal with ductular proliferation, biliary peace-meal necrosis in periportal area. Rare portal granulomas. Lipid-laden macrophages (xanthomas) and lipid-laden hepatocytes (pseudoxanthomas). Vanished interlobular bile ducts. |
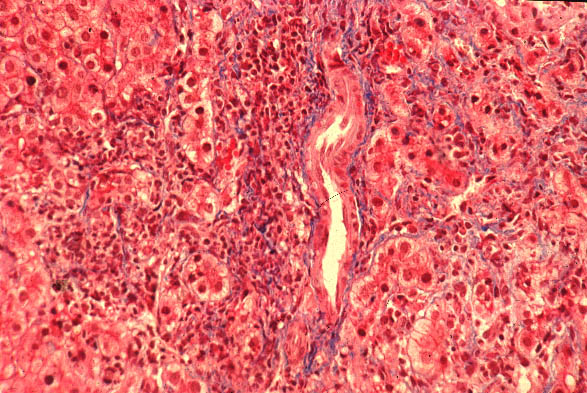
STAGE III
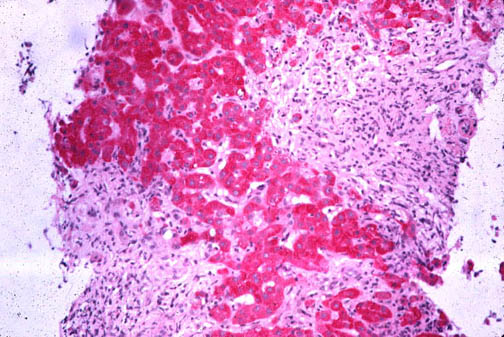 Fig.
11-5-5.Fibrosis, portal, periportal and bridging. Fig.
11-5-5.Fibrosis, portal, periportal and bridging.
This is a wedge biopsy of the liver in a 53 Y/o female Who had hemigastrectomy for peptic ulcer of the stomach. Alk Phos=1000; Pos. AMA=1:600. The biopsy shows portal fibrosis and porto-portal bridges. |
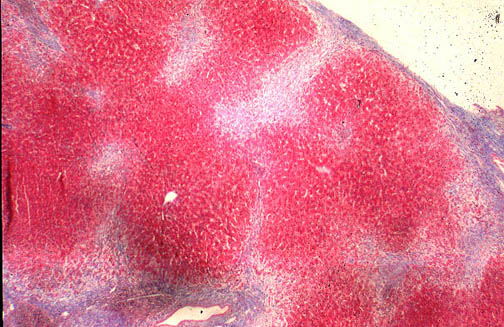 Fig.11-5-6.
Wedge biopsy of stage III. Fig.11-5-6.
Wedge biopsy of stage III.
The fibrous septa are typically devoid of bile ducts. The inflammation is markedly decreased. Granulomas are rarely seen at this stage. Biliary peace-meal necrosis my persist around portal areas and along fibrous septa producing clear halo effect. Mallory bodies, cholestasis and copper granules may be present in periportal areas. |
STAGE IV
Passage from fibrosis to the irreversible changes of cirrhosis consisting of rearrangement of the circulation and of regenerative nodules.
Clinical Features
Sex: 90% more frequent in females. F:M=15:1
Age: Middle age females. Range 22 to 72. Ages 40 to 60 are the most affected.
Distribution: Global
Heredity: Family clustering has been observed
.
Symptoms: The onset of this disease is insidious. The first symptom is usually a disturbing pruritus aggravated by warm weather, night rest, pregnancy and hormones for birth control which may cause a cholestatic damage of the liver. The other symptom is jaundice which may appear months and years, up to 10-20 years, after the pruritus. It rarely appears together or before the pruritus. Jaundice without itching may occur but it is rare. Pigmentation of the skin and xanthomas especially in form of xanthelasmas are a common initial clinical finding. As the disease progresses into fibrosis and cirrhosis, the signs of portal hypertension appear. Some patients may be asymptomatic with liver function tests minimally abnormal but the mitochondrial antibodies will be positive and the histology will be abnormal.
Liver function tests
Serum bilirubin is mildly elevated at the outset (2-4mg).It may remain actually normal for months apparently because not all portal areas are significantly affected.. Serum alkaline phosphatase is markedly increased (up to 4 folds) in symptomatic patients. It may be normal in asymptomatic cases.. Transaminases are mildly elevated. Serum cholesterol may increase but not constantly. Low-density serum lipoproteins are increased due to presence of lipoprotein X which is a protein rich in non-esterified cholesterol. Serum immunoglobulins are up. IgM is elevated in 80% of cases at the earliest stage. There is usually marked increase erythrocyte sedimentation rate.
Immunology:
Search for Anti-Mitochondrial Antibodies is the crucial test for the diagnosis of PBC. There is probably no person affected by this disorder that does not have M-antibodies. These antibodies, directed to the various antigens of the mitochondrion, are obvious multiple, heterogeneous. A group of investigators ( Berg et all) have been characterized
characterized nine types four of which are present in patients affected by PBC. These are: anti-M2, anti-M4, anti-M8 and anti-M9..Anti-M2 is found in all patients with PBC. These antibodies are also found in 30% of autoimmune hepatitis a in some patient with connective tissue disease. They are determined with immunofluorescence and with ELISA technique.
Cholangiography:
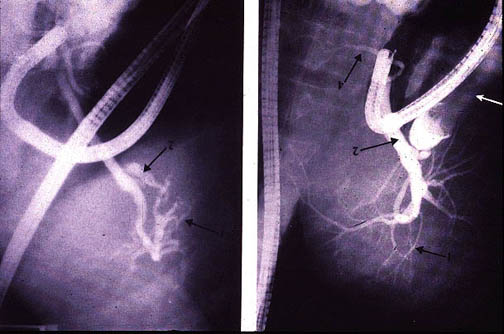 Fig.
11-5-7. Fig.
11-5-7.
The endoscopic retrograde cholangiogram shows changes in the very small intrahepatic bile ducts. At the beginning they are smoothly tapering, then, as they are destroyed, the fine terminations disappear. The large bile ducts are unaffected. The biliary tree appears to have been "pruned". The gall bladder is shrunken and is prone to contain calculi. |
Associated conditions:
In about 69 % of patients PBC may be associated with any other autoimmune disorder and particularly with: systemic lupus erythematosus, rheumatoid arthritis, dermatomyositis, mixed connective tissue disease, rheumatoid arthritis, Scleroderma and CREST syndrome. Dry eyes and mouth (sicca complex) is present in 75% of patients with PBC. Intestinal villous atrophy and ulcerative colitis may also be present.
Prognosis
Asymptomatic patients may have a normal life expectancy. In one study conducted for 11.4 years only 6 out 36 patients died from the liver disease, (Beswick, Gastroenter.89:267,1985). Symptomatic patients with jaundice, hepatosplenomegaly, ascites, hypoalbuminemia, increased prothrombin time and poor histology and presence of associared autoimmune conditions, carry a poor prognosis.
Treatment
Medical treatment include corticosteroids and immunosuppressants.
PBC is the second most common indication for liver transplant which should be done as soon as life- threatening symptoms appear. Survival after transplant is 38.4%. Recurrence has been seen. These patients have higher rate of chronic rejection.